

Flow visualization of a pediatric ventricular assist device during stroke volume reductions related to weaning
- PMID: 21404124
- PMCID: PMC3111892
- DOI: 10.1007/s10439-011-0291-8
Flow visualization of a pediatric ventricular assist device during stroke volume reductions related to weaning
Abstract
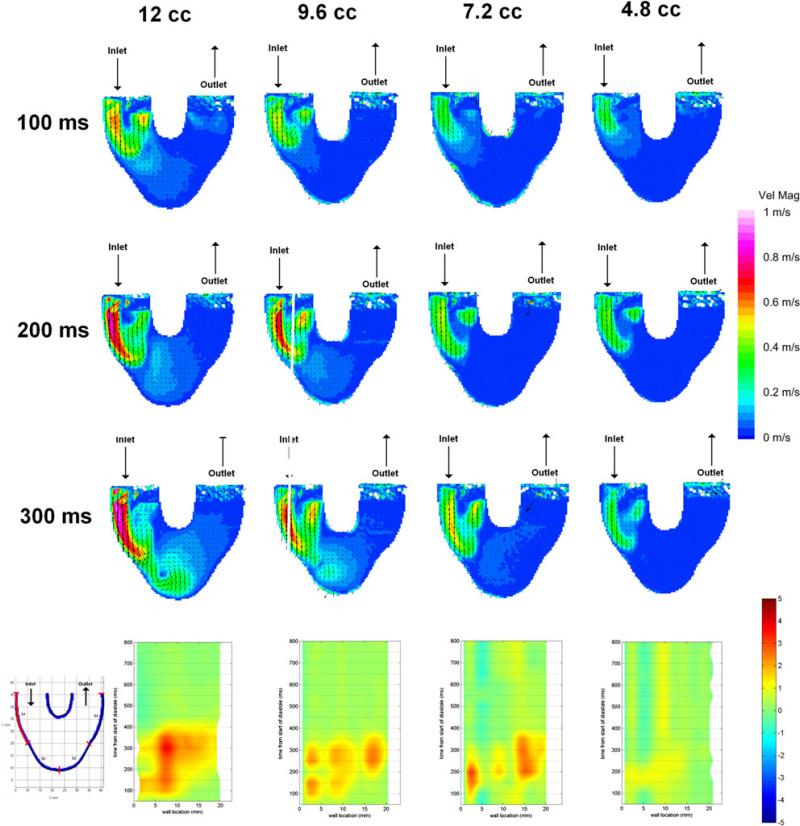
The aim of this study is to define the fluid mechanics of a pulsatile pneumatically driven pediatric ventricular assist device (PVAD), for the reduced flow rates encountered during device weaning and myocardial recovery, and relate the results to the potential for thromboembolic events. We place an acrylic model of the PVAD in a mock circulatory loop filled with a viscoelastic blood analog and operate at four stroke volumes (SVs), each with two different filling conditions, to mimic how the flow rate of the device may be reduced. Particle image velocimetry is used to acquire flow field data. We find that a SV reduction method provides better rotational flow and higher wall shear rates than a beat rate reduction method; that a quick filling condition with a compressed diastolic time is better than a slow filling condition; and, that a reduction in SV to 40% led to greatly reduced fluid movement and wall shear rates that could increase the thrombogenicity of the device. SV reduction is a viable option for flow reduction during weaning, however, it does lead to significant changes to the device flow field and future studies are needed to develop operational protocols for the PVAD during bridge-to-recovery.
Figures











References
-
- Arabia FA, Tsau PH, Smith RG, et al. Pediatric bridge to heart transplantation: application of the berlin heart, medos and thoractec ventricular assist devices. J. Heart Lung Transplant. 2006;25:16–21. - PubMed
-
- Baldwin JT, Deutsch S, Geselowitz DB, Tarbell JM. LDA measurements of mean velocity and reynolds stress fields within an artificial heart ventricle. J. Biomech. Eng. 1994;116:190–200. - PubMed
-
- Cavanaugh JL, Miyamoto SD, da Cruz E, et al. Predicting recovery: successful explant of a ventricular assist device in a child with dilated cardiomyopathy. J. Heart Lung Transplant. 2010;29:105–108. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
