

HIV treatment adherence, drug resistance, virologic failure: evolving concepts
- PMID: 21406048
- PMCID: PMC5072419
- DOI: 10.2174/187152611795589663
HIV treatment adherence, drug resistance, virologic failure: evolving concepts
Abstract
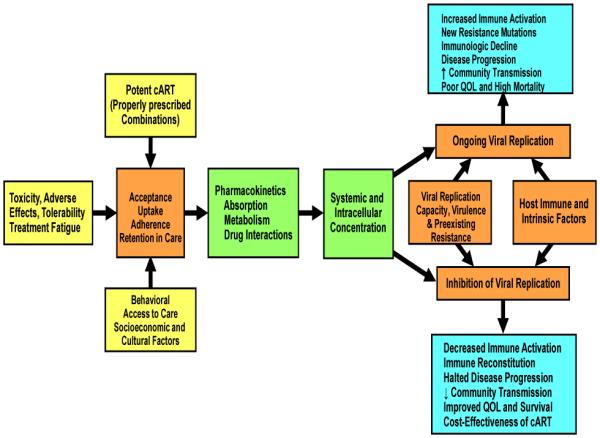
Poor adherence to combined antiretroviral therapy (cART) has been shown to be a major determinant of virologic failure, emergence of drug resistant virus, disease progression, hospitalizations, mortality, and health care costs. While high adherence levels can be achieved in both resource-rich and resource-limited settings following initiation of cART, long-term adherence remains a challenge regardless of available resources. Barriers to optimal adherence may originate from individual (biological, socio-cultural, behavioral), pharmacological, and societal factors. Although patients and providers should continuously strive for maximum adherence to cART, there is accumulating evidence that each class of antiretroviral therapy has specific adherence-drug resistance relationship characteristics allowing certain regimens more flexibility than others. There is not a universally accepted measure for cART adherence, since each method has distinct advantages and disadvantages including cost, complexity, accuracy, precision, intrusiveness and bias. Development of a real-time cART adherence monitoring tool will enable the development of novel, pre-emptive adherence-improving strategies. The application of these strategies may ultimately prove to be the most cost-effective method to reduce morbidity and mortality for the individual and decrease the likelihood of HIV transmission and emergence of resistance in the community.
Figures
References
-
- Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, Wagener MM, Singh N. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann. Intern. Med. 2000;133:21–30. - PubMed
-
- Bangsberg DR. Less than 95% adherence to nonnucleoside reverse-transcriptase inhibitor therapy can lead to viral suppression. Clin. Infect. Dis. 2006;43:939–941. - PubMed
-
- Maggiolo F, Ravasio L, Ripamonti D, Gregis G, Quinzan G, Arici C, Airoldi M, Suter F. Similar adherence rates favor different virologic outcomes for patients treated with nonnucleoside analogues or protease inhibitors. Clin. Infect. Dis. 2005;40:158–163. - PubMed
-
- Nachega JB, Hislop M, Dowdy DW, Chaisson RE, Regensberg L, Maartens G. Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes. Ann. Intern. Med. 2007;146:564–573. - PubMed
-
- Shuter J, Sarlo JA, Kanmaz TJ, Rode RA, Zingman BS. HIV-infected patients receiving lopinavir/ritonavir-based antiretroviral therapy achieve high rates of virologic suppression despite adherence rates less than 95% J. Acquir. Immune Defic. Syndr. 2007;45:4–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K01 AI067063/AI/NIAID NIH HHS/United States
- P30 AI45008/AI/NIAID NIH HHS/United States
- L30 AI080268-02/AI/NIAID NIH HHS/United States
- K23 AI 068582-01/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- R34 MH083592-01A1/MH/NIMH NIH HHS/United States
- K01-AI067063/AI/NIAID NIH HHS/United States
- T32 AI007438/AI/NIAID NIH HHS/United States
- T32 AI007438-16/AI/NIAID NIH HHS/United States
- K23 AI068582/AI/NIAID NIH HHS/United States
- U18 HS016946/HS/AHRQ HHS/United States
- L30 AI080268/AI/NIAID NIH HHS/United States
- R21 MH083592/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
