

Delayed β-cell response and glucose intolerance in young women with Turner syndrome
- PMID: 21406078
- PMCID: PMC3068952
- DOI: 10.1186/1472-6823-11-6
Delayed β-cell response and glucose intolerance in young women with Turner syndrome
Abstract
Background: To investigate glucose homeostasis in detail in Turner syndrome (TS), where impaired glucose tolerance (IGT) and type 2 diabetes are frequent.
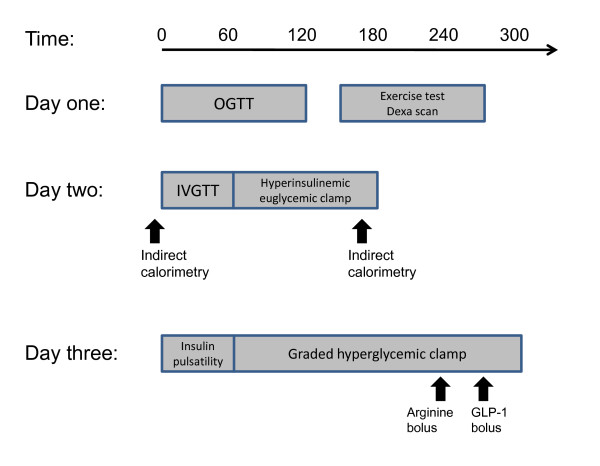
Methods: Cross sectional study of women with Turner syndrome (TS)(n = 13) and age and body mass index matched controls (C) (n = 13), evaluated by glucose tolerance (oral and intravenous glucose tolerance test (OGTT and IVGTT)), insulin sensitivity (hyperinsulinemic, euglycemic clamp), beta-cell function (hyperglycaemic clamp, arginine and GLP-1 stimulation) and insulin pulsatility.
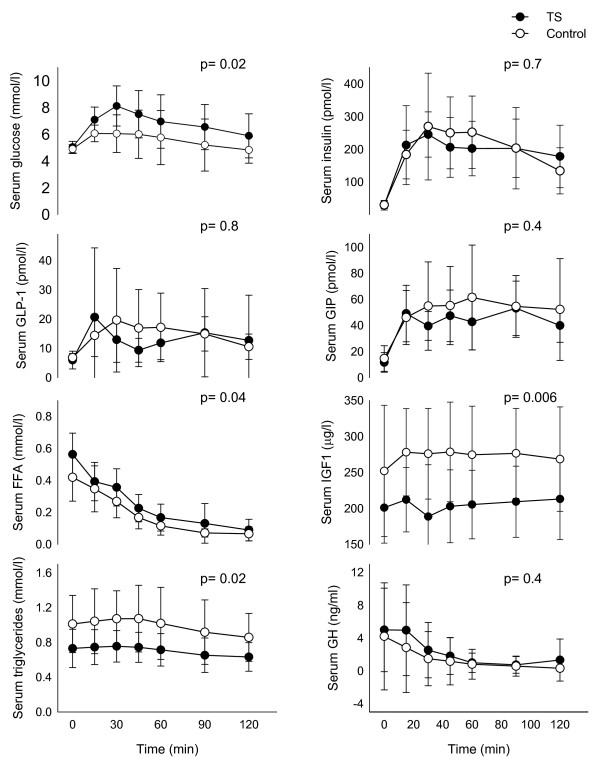
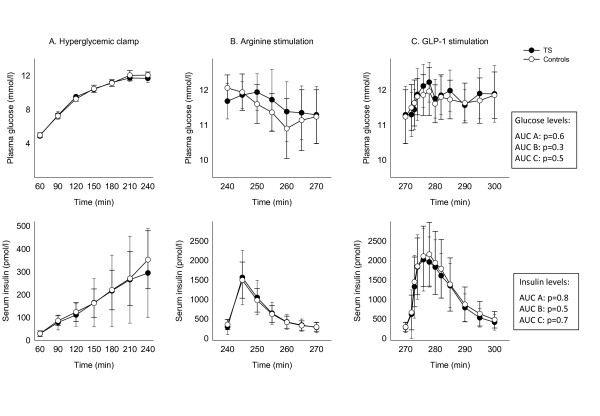
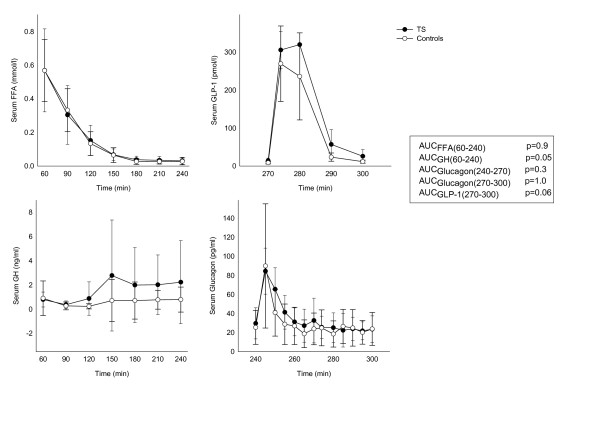
Results: Fasting glucose and insulin levels were similar. Higher glucose responses was seen in TS during OGTT and IVGTT, persisting after correction for body weight or muscle mass, while insulin responses were similar in TS and C, despite the higher glucose level in TS, leading to an insufficient increase in insulin response during dynamic testing. Insulin sensitivity was comparable in the two groups (TS vs. control: 8.6 ± 1.8 vs. 8.9 ± 1.8 mg/kg*30 min; p = 0.6), and the insulin responses to dynamic β-cell function tests were similar. Insulin secretion patterns examined by deconvolution analysis, approximate entropy, spectral analysis and autocorrelation analysis were similar. In addition we found low IGF-I, higher levels of cortisol and norepinephrine and an increased waist-hip ratio in TS.
Conclusions: Young normal weight TS women show significant glucose intolerance in spite of normal insulin secretion during hyperglycaemic clamping and normal insulin sensitivity. We recommend regularly testing for diabetes in TS.
Trial registration: Registered with http://clinicaltrials.com, ID nr: NCT00419107.
Figures
References
-
- Forbes AP, Engel E. The high incidence of diabetes mellitus in 41 patients with gonadal dysgenesis, and their close relatives. Metabolism. 1963;12:428–439. - PubMed
-
- Nielsen J, Johansen K, Yde H. The frequency of diabetes mellitus in patients with Turner's syndrome and pure gonadal dysgenesis. Blood glucose, plasma insulin and growth hormone level during an oral glucose tolerance test. Acta Endocrinol Copenh. 1969;62:251–269. - PubMed
-
- Gravholt CH, Naeraa RW, Nyholm B, Gerdes LU, Christiansen E, Schmitz O, Christiansen JS. Glucose metabolism, lipid metabolism, and cardiovascular risk factors in adult Turner's syndrome. The impact of sex hormone replacement. Diabetes Care. 1998;21:1062–1070. doi: 10.2337/diacare.21.7.1062. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
