

Alcohol intake and risk of oesophageal adenocarcinoma: a pooled analysis from the BEACON Consortium
- PMID: 21406386
- PMCID: PMC3439838
- DOI: 10.1136/gut.2010.233866
Alcohol intake and risk of oesophageal adenocarcinoma: a pooled analysis from the BEACON Consortium
Abstract
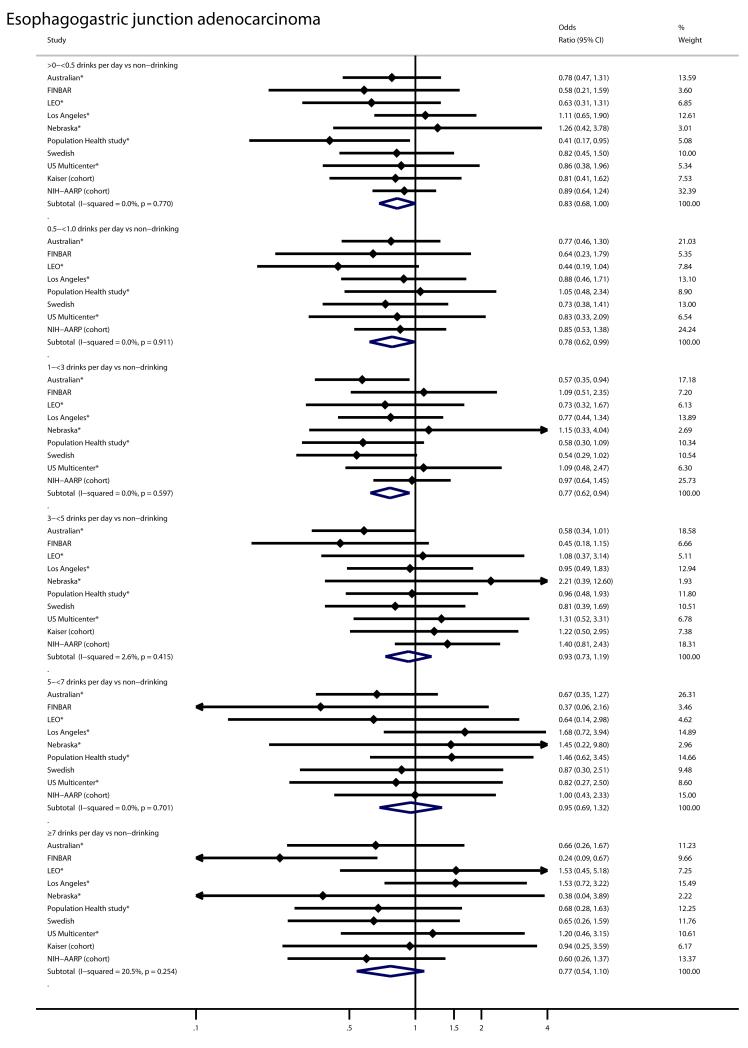
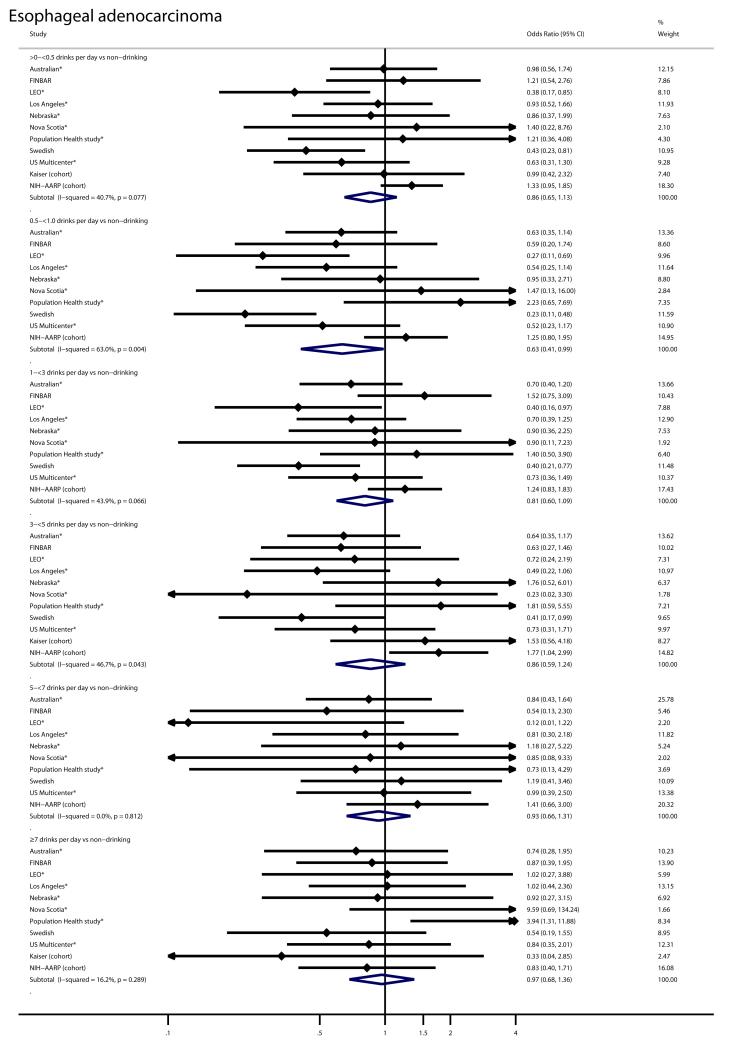
Background and aims: Alcohol intake is a strong and well established risk factor for oesophageal squamous cell carcinoma (OSCC), but the association with oesophageal adenocarcinoma (OA) or adjacent tumours of the oesophagogastric junction (OGJA), remains unclear. Therefore, the association of alcohol intake with OSCC, OA, and OGJA was determined in nine case-control studies and two cohort studies of the Barrett's Esophagus and Esophageal Adenocarcinoma Consortium (BEACON).
Materials and methods: Information was collected on alcohol intake, age, sex, education, body mass index, gastro-oesophageal reflux, and tobacco smoking from each study. Along with 10,854 controls, 1821 OA, and 1837 OGJA, seven studies also collected OSCC cases (n=1016). Study specific ORs and 95% CIs were calculated from multivariate adjusted logistic regression models for alcohol intake in categories compared to non-drinkers. Summary risk estimates were obtained by random effects models. Results No increase was observed in the risk of OA or OGJA for increasing levels of any of the alcohol intake measures examined. ORs for the highest frequency category (≥ 7 drinks per day) were 0.97 (95% CI 0.68 to 1.36) for OA and 0.77 (95% CI = 0.54 to 1.10) for OGJA. Suggestive findings linked moderate intake (eg, 0.5 to <1 drink per day) to decreased risk of OA (OR 0.63, 95% CI 0.41 to 0.99) and OGJA (OR 0.78, 95% CI 0.62 to 0.99). In contrast, alcohol intake was strongly associated with increased risk of OSCC (OR for ≥ 7 drinks per day 9.62, 95% CI 4.26 to 21.71).
Conclusions: In contrast to OSCC, higher alcohol consumption was not associated with increased risk of either OA or OGJA. The apparent inverse association observed with moderate alcohol intake should be evaluated in future prospective studies.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349:2241–52. - PubMed
-
- Brown LM, Hoover RN, Greenberg RS, et al. Are racial differences in squamous cell esophageal cancer explained by alcohol and tobacco use? J Natl Cancer Inst. 1994;86:1340–5. - PubMed
-
- Castellsague X, Munoz N, De SE, et al. Independent and joint effects of tobacco smoking and alcohol drinking on the risk of esophageal cancer in men and women. Int J Cancer. 1999;82:657–64. - PubMed
Publication types
MeSH terms
Grants and funding
- R21DKO77742/PHS HHS/United States
- R01 AI057947/AI/NIAID NIH HHS/United States
- CA59636/CA/NCI NIH HHS/United States
- R01 DK063616/DK/NIDDK NIH HHS/United States
- R01 CA57947-03/CA/NCI NIH HHS/United States
- U01 CA057923/CA/NCI NIH HHS/United States
- R37-CA41530/CA/NCI NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- R21 DK077742/DK/NIDDK NIH HHS/United States
- P30 ES010126/ES/NIEHS NIH HHS/United States
- K05 CA124911/CA/NCI NIH HHS/United States
- R01-CA30022/CA/NCI NIH HHS/United States
- U01 CA057949/CA/NCI NIH HHS/United States
- R01 CA030022/CA/NCI NIH HHS/United States
- U01 CA057983/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical