

Overcoming temozolomide resistance in glioblastoma via dual inhibition of NAD+ biosynthesis and base excision repair
- PMID: 21406402
- PMCID: PMC3077901
- DOI: 10.1158/0008-5472.CAN-10-3213
Overcoming temozolomide resistance in glioblastoma via dual inhibition of NAD+ biosynthesis and base excision repair
Abstract
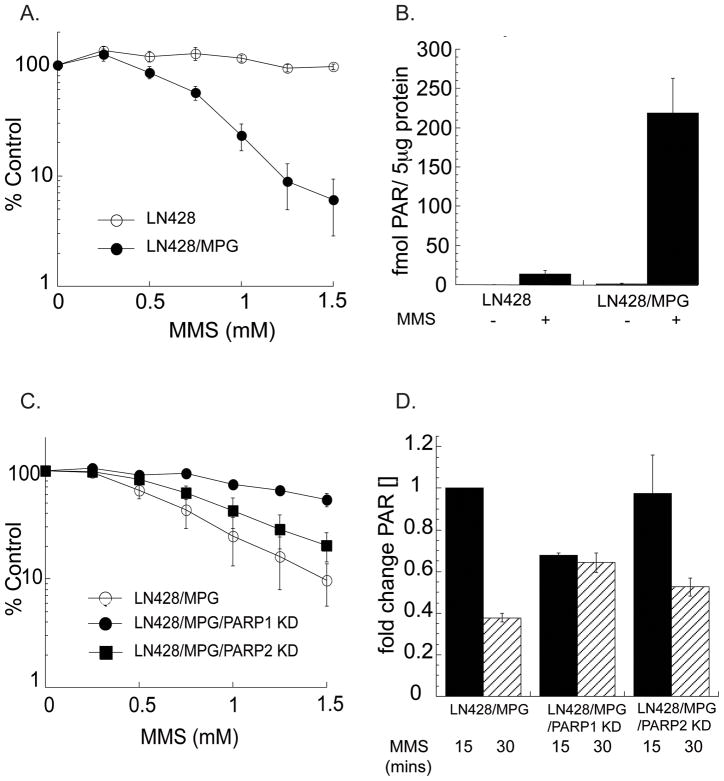
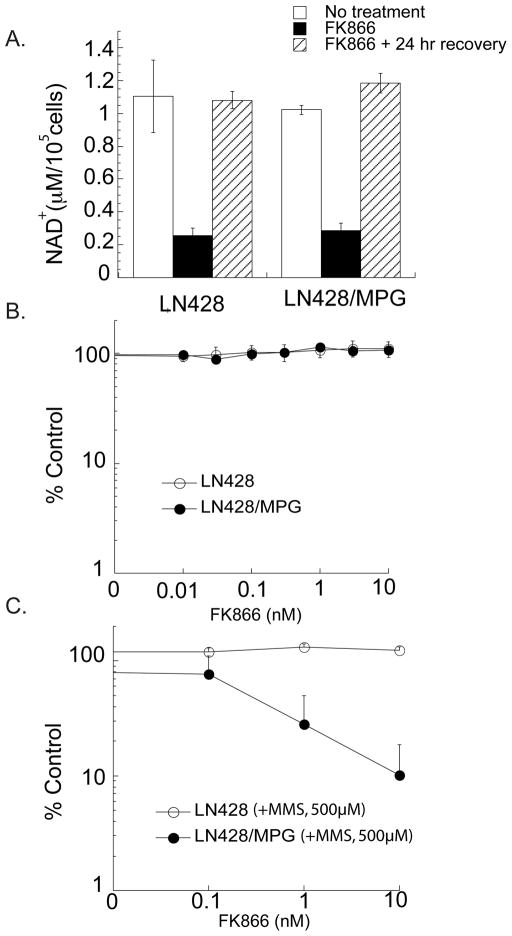
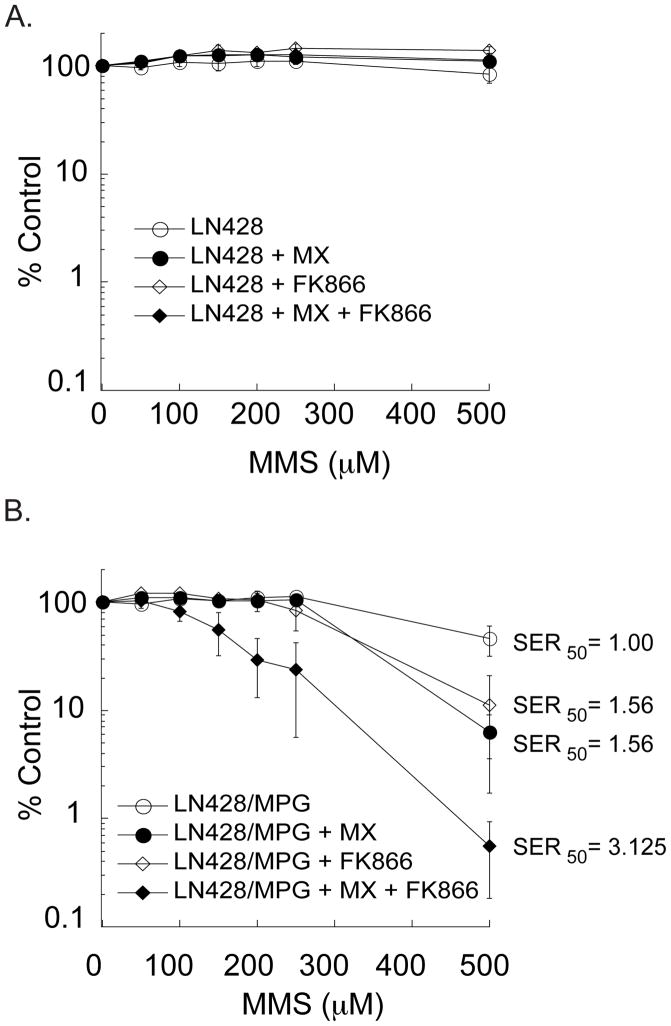
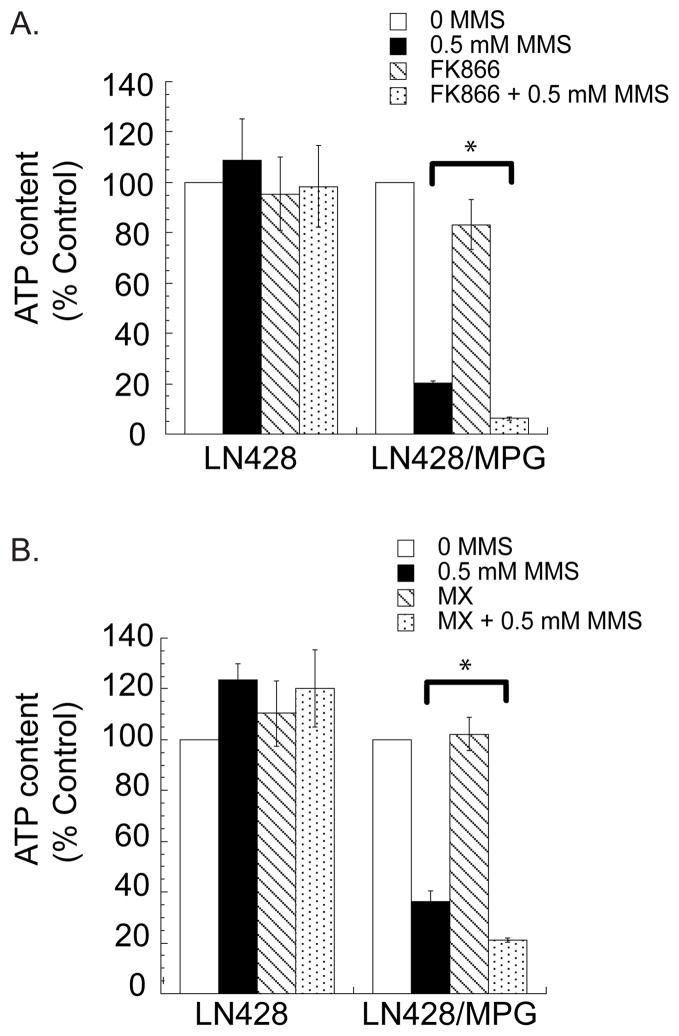
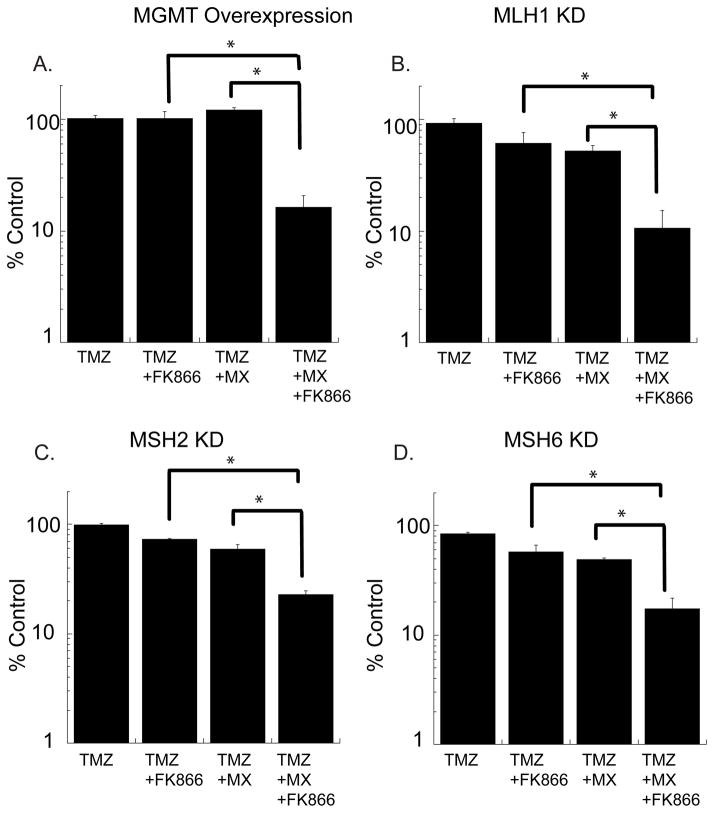
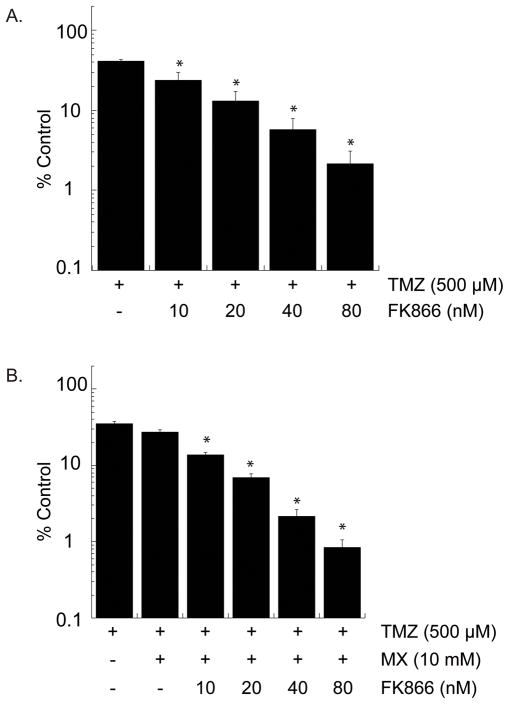
Glioblastoma multiforme (GBM) is a devastating brain tumor with poor prognosis and low median survival time. Standard treatment includes radiation and chemotherapy with the DNA alkylating agent temozolomide (TMZ). However, a large percentage of tumors are resistant to the cytotoxic effects of the TMZ-induced DNA lesion O(6)-methylguanine due to elevated expression of the repair protein O(6)-methylguanine-DNA methyltransferase (MGMT) or a defect in the mismatch repair (MMR) pathway. Although a majority of the TMZ-induced lesions (N7-methylguanine and N3-methyladenine) are base excision repair (BER) substrates, these DNA lesions are also readily repaired. However, blocking BER can enhance response to TMZ and therefore the BER pathway has emerged as an attractive target for reversing TMZ resistance. Our lab has recently reported that inhibition of BER leads to the accumulation of repair intermediates that induce energy depletion-mediated cell death via hyperactivation of poly(ADP-ribose) polymerase. On the basis of our observation that TMZ-induced cell death via BER inhibition is dependent on the availability of nicotinamide adenine dinucleotide (NAD(+)), we have hypothesized that combined BER and NAD(+) biosynthesis inhibition will increase TMZ efficacy in glioblastoma cell lines greater than BER inhibition alone. Importantly, we find that the combination of BER and NAD(+) biosynthesis inhibition significantly sensitizes glioma cells with elevated expression of MGMT and those deficient in MMR, two genotypes normally associated with TMZ resistance. Dual targeting of these two interacting pathways (DNA repair and NAD(+) biosynthesis) may prove to be an effective treatment combination for patients with resistant and recurrent GBM.
© 2011 AACR.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
References
-
- Sathornsumetee S, Rich JN. New treatment strategies for malignant gliomas. Expert Rev Anticancer Ther. 2006;6:1087–104. - PubMed
-
- Friedman HS, Kerby T, Calvert H. Temozolomide and treatment of malignant glioma. Clinical Cancer Research. 2000;6:2585–97. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New England Journal of Medicine. 2005;352:987–96. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–66. - PubMed
-
- Sobol RW. Temozolomide. In: Schwab M, editor. Encyclopedia of Cancer. 2. Berlin, Heidelberg, New York: Springer; 2009.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
