

Saliva/pathogen biomarker signatures and periodontal disease progression
- PMID: 21406610
- PMCID: PMC3144122
- DOI: 10.1177/0022034511399908
Saliva/pathogen biomarker signatures and periodontal disease progression
Erratum in
- J Dent Res. 2011 Aug;90(8):1037
Abstract
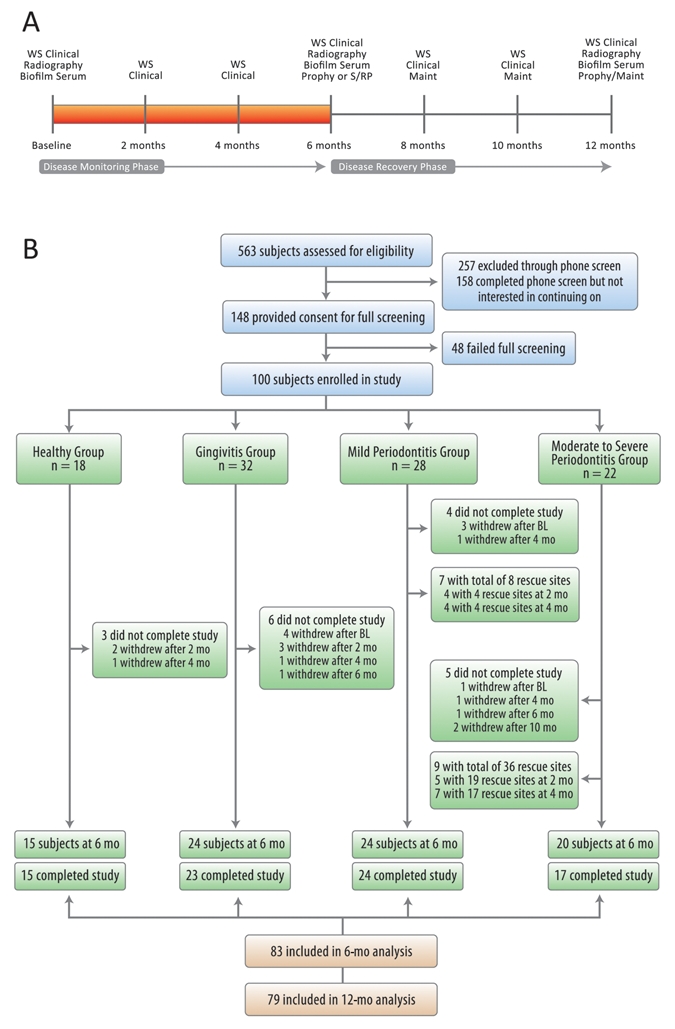
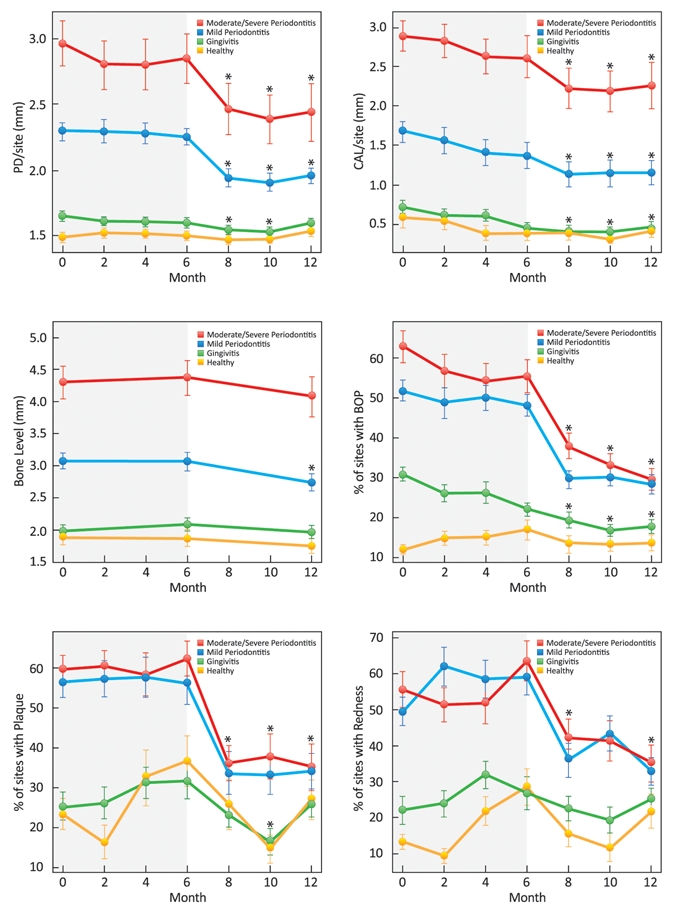
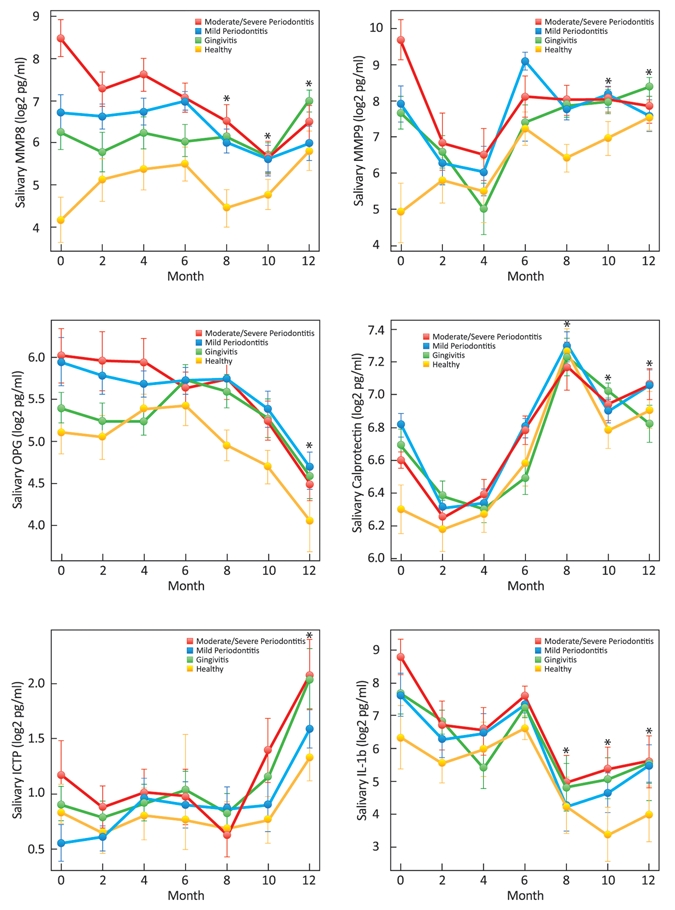
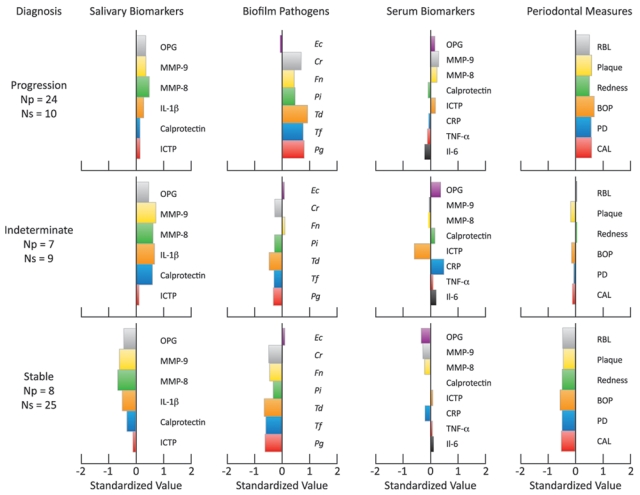
The purpose of this study was to determine the role of saliva-derived biomarkers and periodontal pathogens during periodontal disease progression (PDP). One hundred human participants were recruited into a 12-month investigation. They were seen bi-monthly for saliva and clinical measures and bi-annually for subtraction radiography, serum and plaque biofilm assessments. Saliva and serum were analyzed with protein arrays for 14 pro-inflammatory and bone turnover markers, while qPCR was used for detection of biofilm. A hierarchical clustering algorithm was used to group study participants based on clinical, microbiological, salivary/serum biomarkers, and PDP. Eighty-three individuals completed the six-month monitoring phase, with 39 [corrected] exhibiting PDP, while 44 [corrected] demonstrated stability. Participants assembled into three clusters based on periodontal pathogens, serum and salivary biomarkers. Cluster 1 members displayed high salivary biomarkers and biofilm; 71% [corrected] of these individuals were undergoing PDP. Cluster 2 members displayed low biofilm and biomarker levels; 76% [corrected] of these individuals were stable. Cluster 3 members were not discriminated by PDP status; however, cluster stratification followed groups 1 and 2 based on thresholds of salivary biomarkers and biofilm pathogens. The association of cluster membership to PDP was highly significant (p < 0.0007). [corrected] The use of salivary and biofilm biomarkers offers potential for the identification of PDP or stability (ClinicalTrials.gov number, CT00277745).
Trial registration: ClinicalTrials.gov NCT00277745.
Figures
References
-
- Armitage GC. (1999). Development of a classification system for periodontal diseases and conditions. Ann Periodontol 4:1-6 - PubMed
-
- Bassim CW, Redman RS, DeNucci DJ, Becker KL, Nyler ES. (2008). Salivary procalcitonin and periodontitis in diabetes. J Dent Res 87:630-4 - PubMed
-
- Christodoulides N, Floriano PN, Miller CS, Ebersole JL, Mohanty S, Dharshan P, et al. (2007). Lab-on-a-chip methods for point-of-care measurements of salivary biomarkers of periodontitis. Ann NY Acad Sci 1098:411-428 - PubMed
-
- Darveau RP. (2010). Periodontitis: a polymicrobial disruption of host homeostasis. Nat Rev Microbiol 8:481-490 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
