

SERCA2a gene transfer decreases sarcoplasmic reticulum calcium leak and reduces ventricular arrhythmias in a model of chronic heart failure
- PMID: 21406682
- PMCID: PMC3119354
- DOI: 10.1161/CIRCEP.110.961615
SERCA2a gene transfer decreases sarcoplasmic reticulum calcium leak and reduces ventricular arrhythmias in a model of chronic heart failure
Abstract
Background: Sarcoplasmic reticulum calcium ATPase 2a (SERCA2a) gene therapy improves mechanical function in heart failure and is under evaluation in a clinical trial. A critical question is whether SERCA2a gene therapy predisposes to increased sarcoplasmic reticulum calcium (SR Ca(2+)) leak, cellular triggered activity, and ventricular arrhythmias in the failing heart.
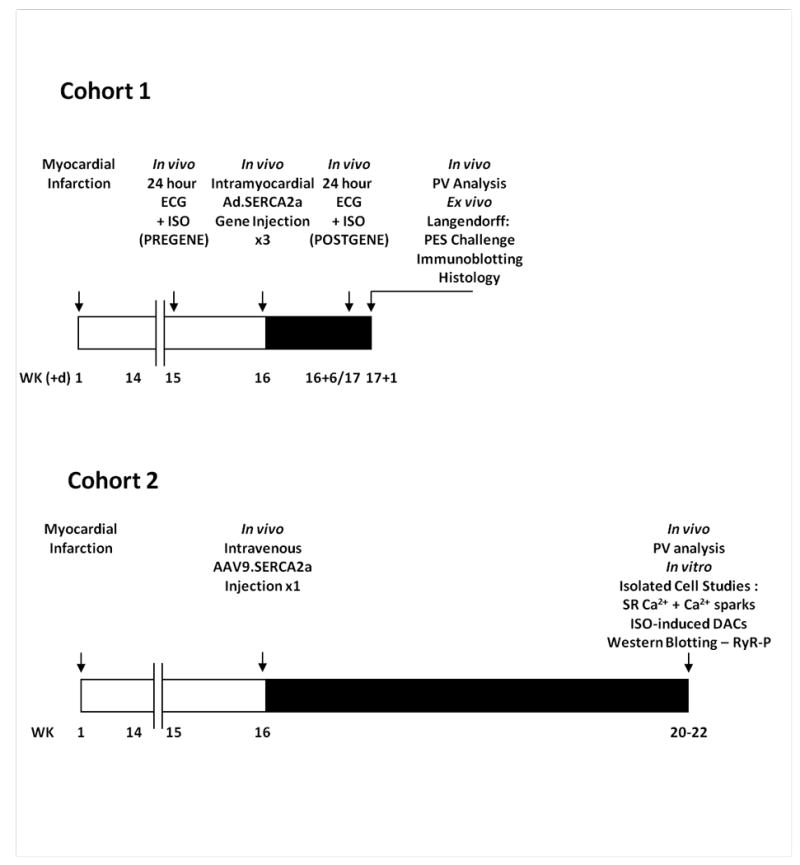
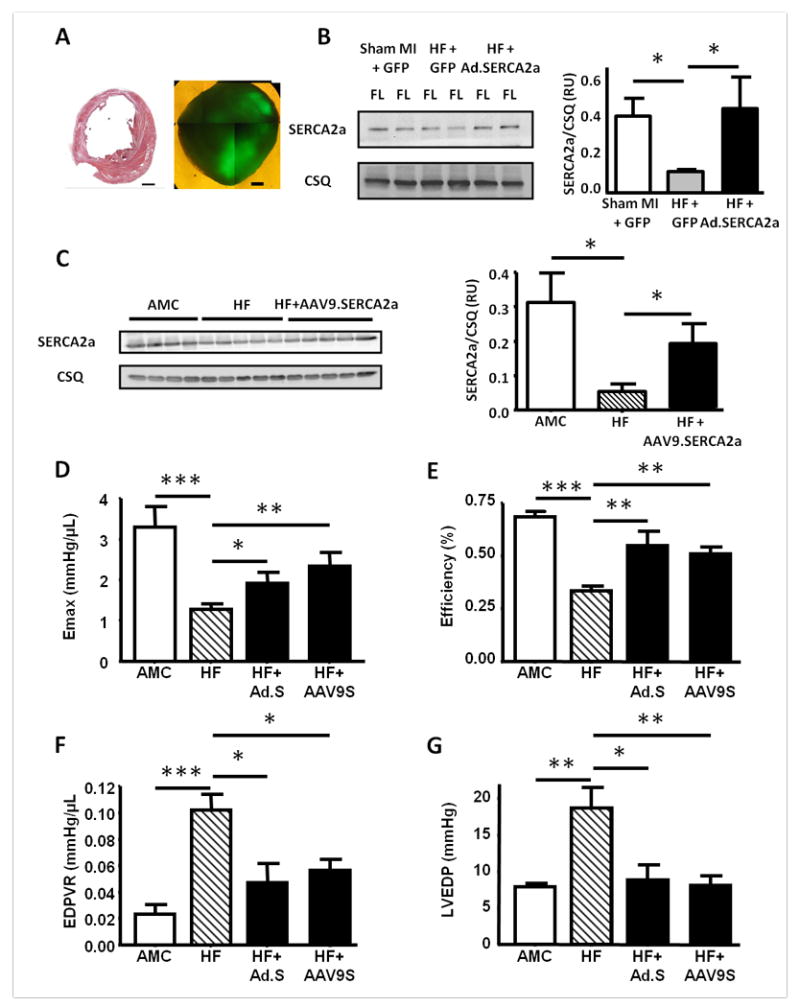
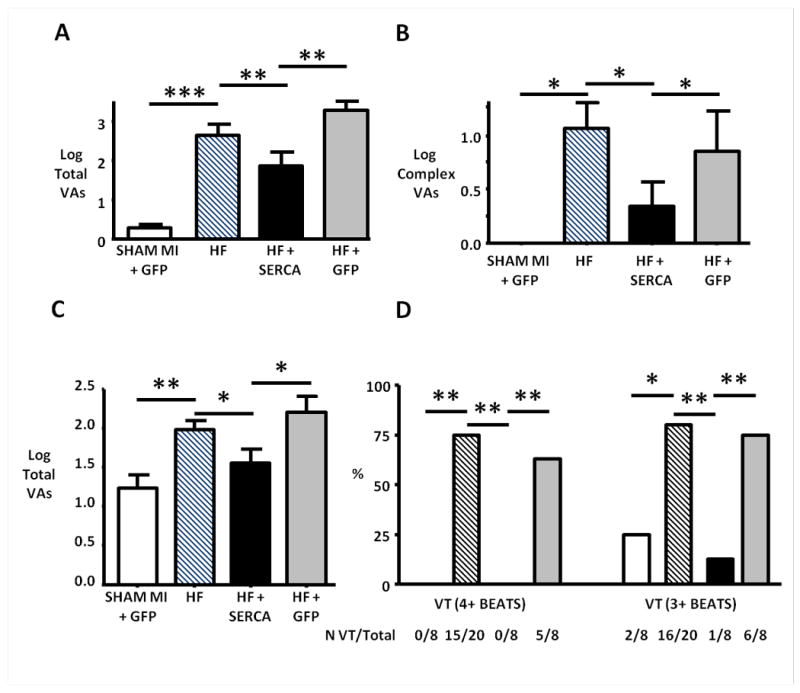
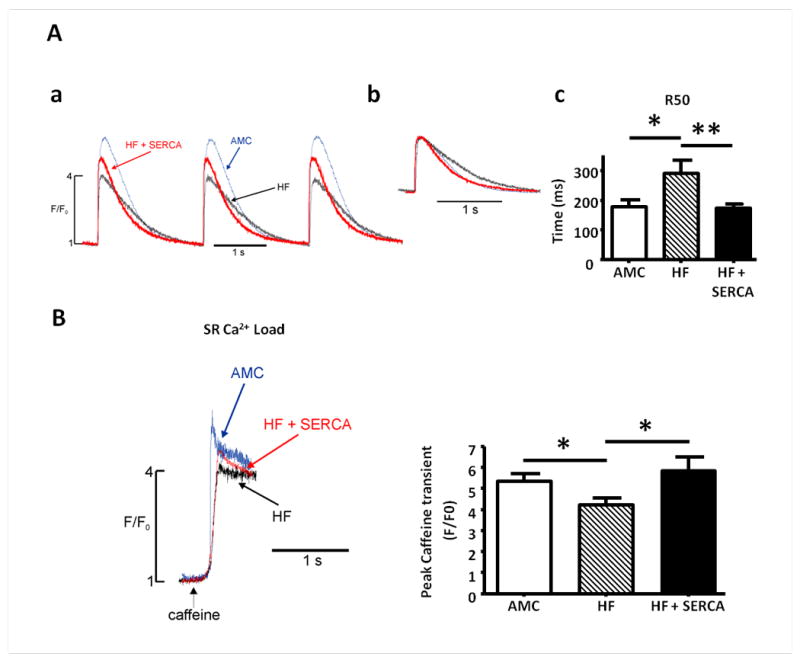
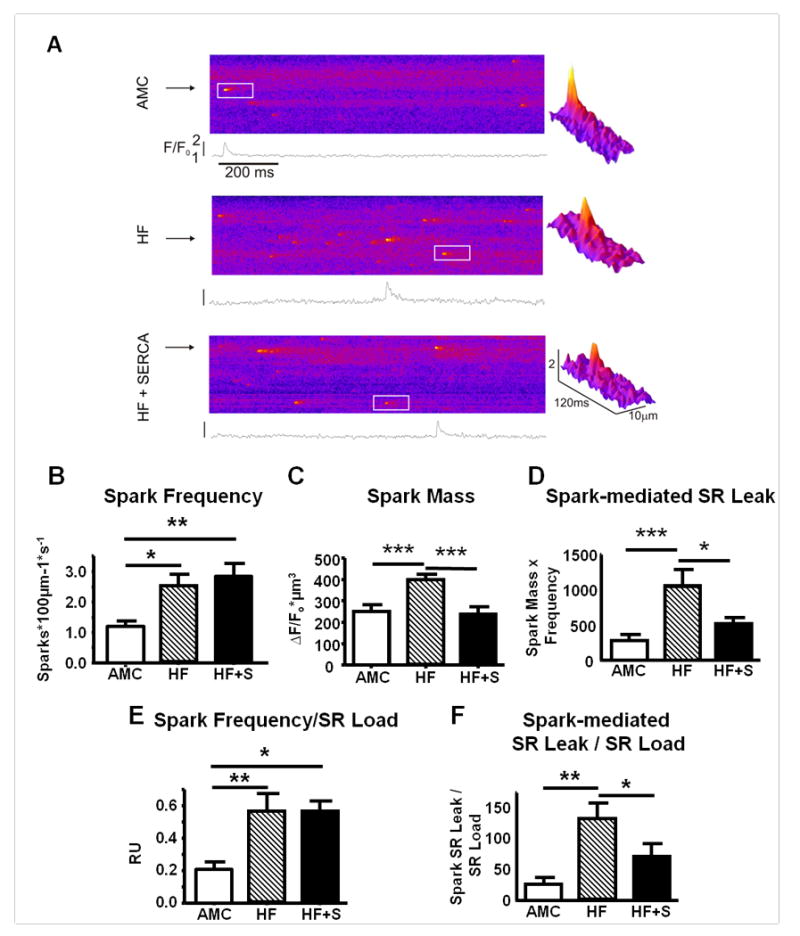
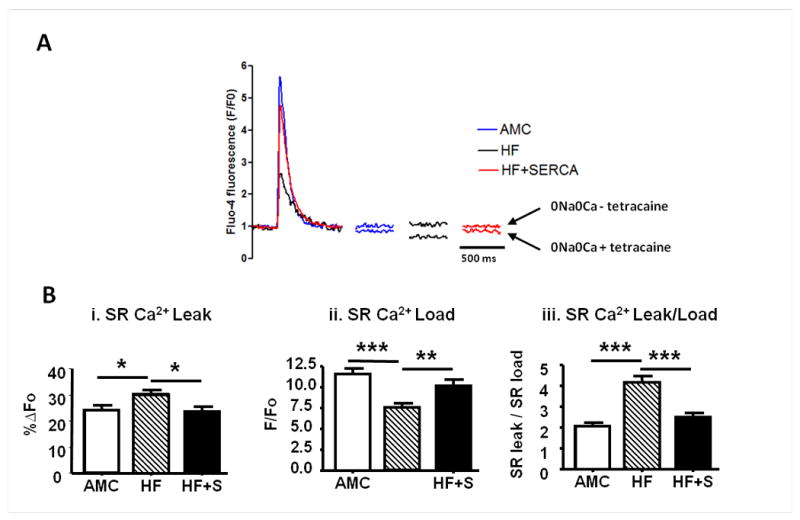
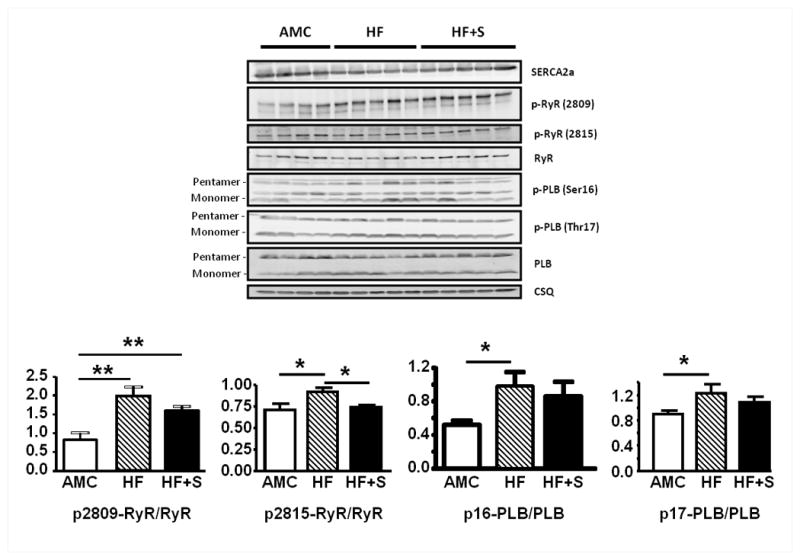
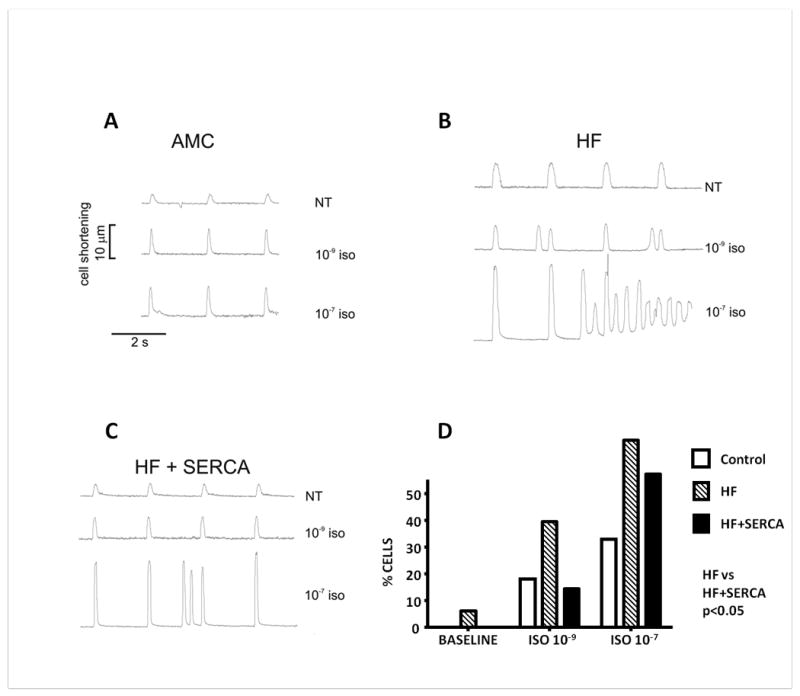
Methods and results: We studied the influence of SERCA2a gene therapy on ventricular arrhythmogenesis in a rat chronic heart failure model. ECG telemetry studies revealed a significant antiarrhythmic effect of SERCA2a gene therapy with reduction of both spontaneous and catecholamine-induced arrhythmias in vivo. SERCA2a gene therapy also reduced susceptibility to reentry arrhythmias in ex vivo programmed electrical stimulation studies. Subcellular Ca(2+) homeostasis and spontaneous SR Ca(2+) leak characteristics were measured in failing cardiomyocytes transfected in vivo with a novel AAV9.SERCA2a vector. SR Ca(2+) leak was reduced after SERCA2a gene therapy, with reversal of the greater spark mass observed in the failing myocytes, despite normalization of SR Ca(2+) load. SERCA2a reduced ryanodine receptor phosphorylation, thereby resetting SR Ca(2+) leak threshold, leading to reduced triggered activity in vitro. Both indirect effects of reverse remodeling and direct SERCA2a effects appear to underlie the antiarrhythmic action.
Conclusions: SERCA2a gene therapy stabilizes SR Ca(2+) load, reduces ryanodine receptor phosphorylation and decreases SR Ca(2+) leak, and reduces cellular triggered activity in vitro and spontaneous and catecholamine-induced ventricular arrhythmias in vivo in failing hearts. SERCA2a gene therapy did not therefore predispose to arrhythmias and may represent a novel antiarrhythmic strategy in heart failure.
Conflict of interest statement
Figures
References
-
- Kawase Y, Ly HQ, Prunier F, Lebeche D, Shi Y, Jin H, Hadri L, Yoneyama R, Hoshino K, Takewa Y, Sakata S, Peluso R, Zsebo K, Gwathmey JK, Tardif JC, Tanguay JF, Hajjar RJ. Reversal of Cardiac Dysfunction After Long-Term Expression of SERCA2a by Gene Transfer in a Pre-Clinical Model of Heart Failure. J Am Coll Cardiol. 2008;51:1112–9. - PubMed
-
- Byrne MJ, Power JM, Preovolos A, Mariani JA, Hajjar RJ, Kaye DM. Recirculating cardiac delivery of AAV2/1SERCA2a improves myocardial function in an experimental model of heart failure in large animals. Gene Ther. 2008;15:1550–7. - PubMed
-
- Hajjar RJ, Zsebo K, Deckelbaum L, Thompson C, Rudy J, Yaroshinsky A, Ly H, Kawase Y, Wagner K, Borow K, Jaski B, London B, Greenberg B, Pauly DF, Patten R, Starling R, Mancini D, Jessup M. Design of a Phase 1/2 Trial of Intracoronary Administration of AAV1/SERCA2a in Patients With Heart Failure. J Cardiac Failure. 2008;14:355–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
