

Adherence to drug-refill is a useful early warning indicator of virologic and immunologic failure among HIV patients on first-line ART in South Africa
- PMID: 21408071
- PMCID: PMC3052314
- DOI: 10.1371/journal.pone.0017518
Adherence to drug-refill is a useful early warning indicator of virologic and immunologic failure among HIV patients on first-line ART in South Africa
Abstract
Background: Affordable strategies to prevent treatment failure on first-line regimens among HIV patients are essential for the long-term success of antiretroviral therapy (ART) in sub-Saharan Africa. WHO recommends using routinely collected data such as adherence to drug-refill visits as early warning indicators. We examined the association between adherence to drug-refill visits and long-term virologic and immunologic failure among non-nucleoside reverse transcriptase inhibitor (NNRTI) recipients in South Africa.
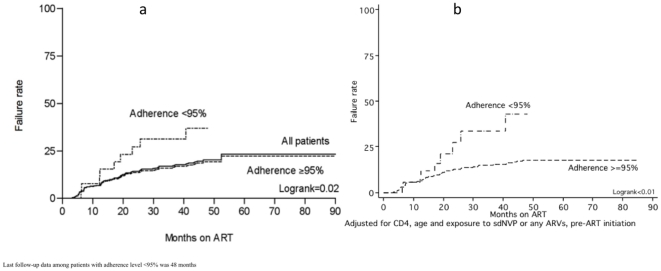
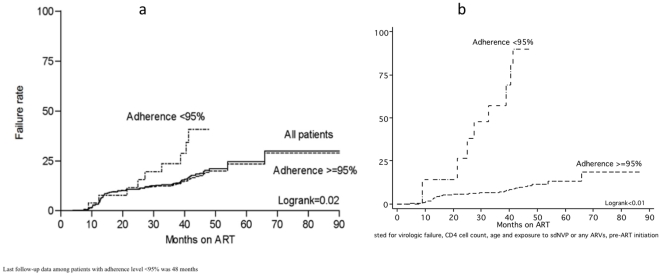
Methods: In 2008, 456 patients on NNRTI-based ART for a median of 44 months (range 12-99 months; 1,510 person-years) were enrolled in a retrospective cohort study in Soweto. Charts were reviewed for clinical characteristics before and during ART. Multivariable logistic regression and Kaplan-Meier survival analysis assessed associations with virologic (two repeated VL>50 copies/ml) and immunologic failure (as defined by WHO).
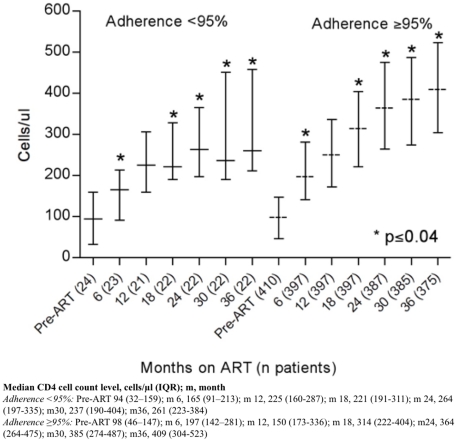
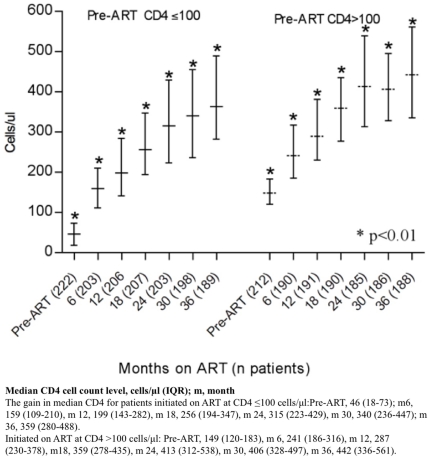
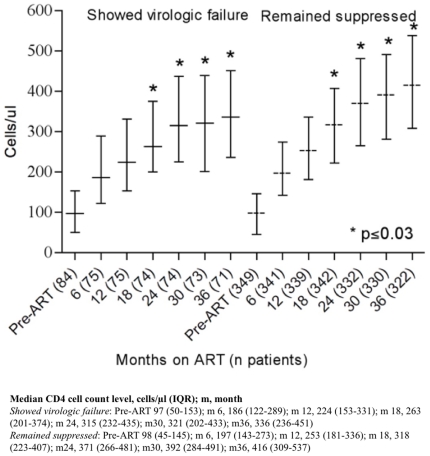
Results: After a median of 15 months on ART, 19% (n = 88) and 19% (n = 87) had failed virologically and immunologically respectively. A cumulative adherence of <95% to drug-refill visits was significantly associated with both virologic and immunologic failure (p<0.01). In the final multivariable model, risk factors for virologic failure were incomplete adherence (OR 2.8, 95%CI 1.2-6.7), and previous exposure to single-dose nevirapine or any other antiretrovirals (adj. OR 2.1, 95%CI 1.2-3.9), adjusted for age and sex. In Kaplan-Meier analysis, the virologic failure rate by month 48 was 19% vs. 37% among adherent and non-adherent patients respectively (logrank p value = 0.02).
Conclusion: One in five failed virologically after a median of 15 months on ART. Adherence to drug-refill visits works as an early warning indicator for both virologic and immunologic failure.
Conflict of interest statement
Figures
References
-
- World Health Organization (WHO), Joint United Nations Programme on HIV/AIDS, UNICEF. Progress report; 2008. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector. pp. 1–77.
-
- Harries AD, Zachariah R, van Oosterhout JJ, Reid SD, Hosseinipour MC, et al. Diagnosis and management of antiretroviral-therapy failure in resource-limited settings in sub-Saharan Africa: challenges and perspectives. Lancet Infect Dis. 2010;10:60–65. - PubMed
-
- Kuritzkes DR. Preventing and managing antiretroviral resistance. AIDS Patient Care STDs. 2004;18:259–273. - PubMed
-
- Calmy A, Ford N, Hirschel B, Reynolds SJ, Lynen L, et al. HIV viral load monitoring in resource-limited regions: optional or necessary? Clin Infect Dis. 2007;44:128–134. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
