

The association of early post-transplant glucose levels with long-term mortality
- PMID: 21409415
- PMCID: PMC3088823
- DOI: 10.1007/s00125-011-2105-9
The association of early post-transplant glucose levels with long-term mortality
Abstract
Aims/objective: We aimed to assess the long-term effects of post-transplant glycaemia on long-term survival after renal transplantation.
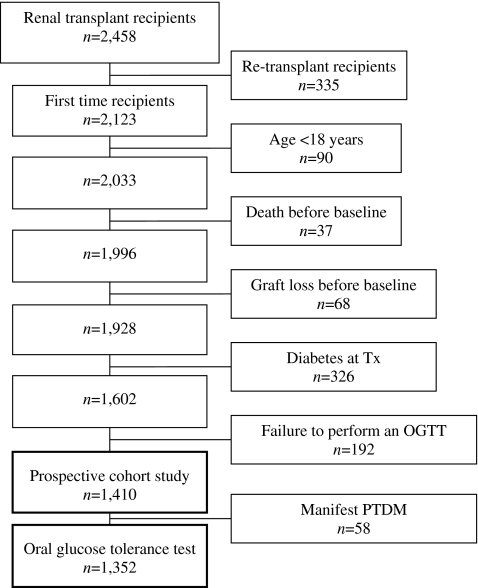
Methods: Study participants were 1,410 consecutive transplant recipients without known diabetes who underwent an OGTT 10 weeks post-transplant and were observed for a median of 6.7 years (range 0.3-13.8 years). The HRs adjusted for age, sex, traditional risk factors and transplant-related risk factors were estimated.
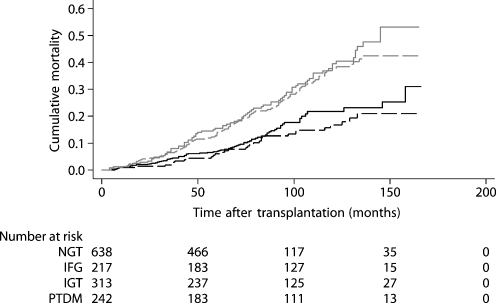
Results: Each 1 mmol/l increase in fasting plasma glucose (fPG) or 2 h plasma glucose (2hPG) was associated with 11% (95% CI -1%, 24%) and 5% (1%, 9%) increments in all-cause mortality risk and 19% (1%, 39%) and 6% (1%, 12%) increments in cardiovascular (CV) mortality risk, respectively. Including both fPG and 2hPG in the multi-adjusted model the HR for 2hPG remained unchanged, while the HR for fPG was attenuated (1.05 [1.00, 1.11] and 0.97 [0.84, 1.14]). Compared with recipients with normal glucose tolerance, patients with post-transplant diabetes mellitus had higher all-cause and CV mortality (1.54 [1.09, 2.17] and 1.80 [1.10, 2.96]), while patients with impaired glucose tolerance (IGT) had higher all-cause, but not CV mortality (1.39 [1.01, 1.91] and 1.04 [0.62, 1.74]). Conversely, impaired fasting glucose was not associated with increased all-cause or CV mortality (0.79 [0.52, 1.23] and 0.76 [0.39, 1.49]). Post-challenge hyperglycaemia predicted death from any cause and infectious disease in the multivariable analyses (1.49 [1.15, 1.95] and 1.91 [1.09, 3.33]).
Conclusions/interpretation: For predicting all-cause and CV mortality, 2hPG is superior to fPG after renal transplantation. Also, early post-transplant diabetes, IGT and post-challenge hyperglycaemia were significant predictors of death. Future studies should determine whether an OGTT helps identify renal transplant recipients at increased risk of premature death.
Figures
References
-
- Kasiske BL, Chakkera HA, Roel J. Explained and unexplained ischemic heart disease risk after renal transplantation. J Am Soc Nephrol. 2000;11:1735–1743. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
