

Case Reports
doi: 10.1007/s00167-011-1465-5.
Epub 2011 Mar 16.
Tertiary osteochondral defect of the talus treated by a novel contoured metal implant
Affiliations
- PMID: 21409468
- PMCID: PMC3096766
- DOI: 10.1007/s00167-011-1465-5
Item in Clipboard
Case Reports
Tertiary osteochondral defect of the talus treated by a novel contoured metal implant
Knee Surg Sports Traumatol Arthrosc.
2011 Jun.
Abstract
The primary treatment of most osteochondral defects of the talus is arthroscopic debridement and bone marrow stimulation. There is no optimal treatment for large lesions or for those in which primary treatment has failed. We report a 20-year-old female patient with persistent symptoms after two previous arthroscopic procedures. Computed tomography showed a cystic defect of the medial talar dome, sized 17×8×8 mm. The patient was treated with a novel contoured metal implant. At 1 and 2 years after surgery, the patient reported considerable reduction in pain and had resumed playing korfball at competitive level. Level of evidence IV.
Figures

Preoperative anteroposterior mortise view and lateral radiographs of the affected ankle showing a radiolucent osteochondral defect in the medial talar dome (arrow)
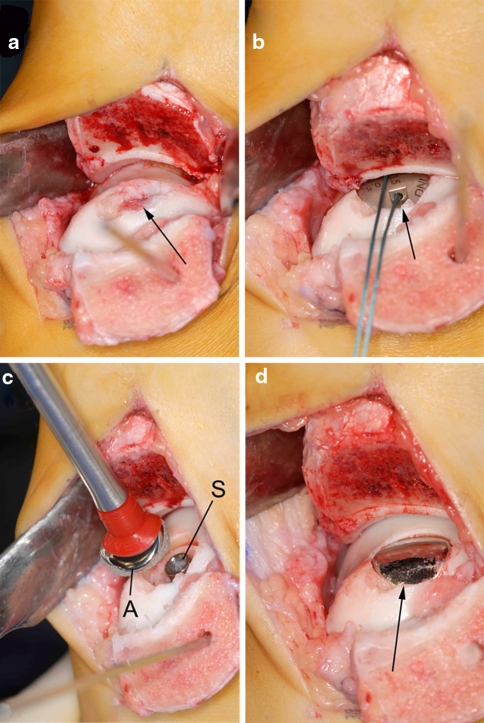
Intraoperative pictures of the operative technique. a The talar lesion was exposed through an oblique medial malleolar osteotomy, and the necrotic fragment was excised (arrow). b After the insertion of a screw and the determination of the appropriate offset sizes, a trial articular component (arrow) was placed. c The final articular component (A) was orientated in the correct plane and placed on the screw (S). d Final view of the talus after engagement of the articular component (arrow). Note that the edges of the implant are slightly recessed compared to the adjacent cartilage level

Radiographs after 2 years follow-up. There are no implant-related complications or progressive degenerative changes of the ankle joint when compared to preoperatively
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
