

Utilization of frequency domain optical coherence tomography and fractional flow reserve to assess intermediate coronary artery stenoses: conciliating anatomic and physiologic information
- PMID: 21409535
- PMCID: PMC3984934
- DOI: 10.1007/s10554-011-9847-9
Utilization of frequency domain optical coherence tomography and fractional flow reserve to assess intermediate coronary artery stenoses: conciliating anatomic and physiologic information
Abstract
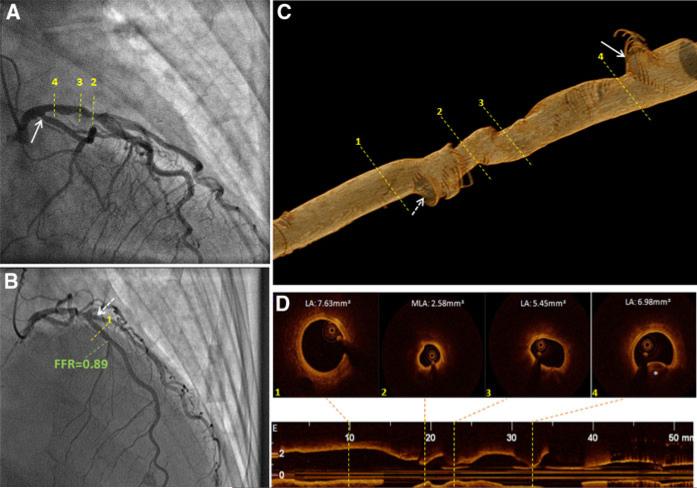
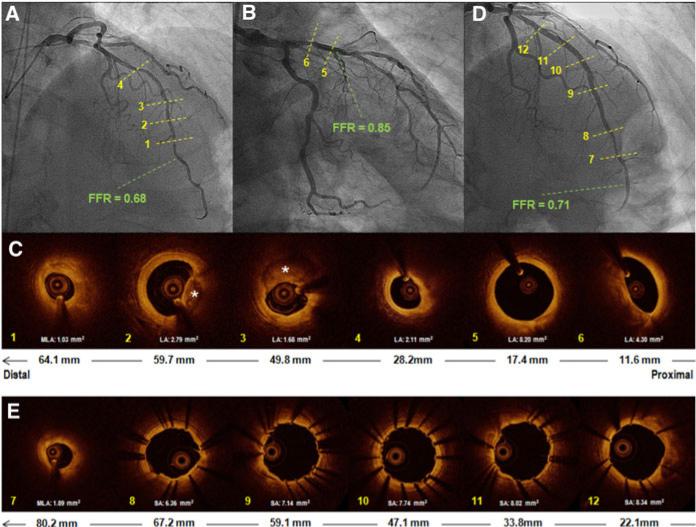
Fractional flow reserve (FFR) and intravascular imaging respectively provide hemodynamic and anatomical assessments of angiographic intermediate stenoses. Frequency domain optical coherence tomography (FD-OCT) is a promising high-resolution imaging modality, but its clinical use in determining severity of coronary disease has yet to be determined. There, we set out to determine the role of FD-OCT to complement FFR in the evaluation of intermediate coronary artery stenoses. FD-OCT was planned in 176 consecutive interventional procedures at our institution to delineate the proper use of FD-OCT in clinical practice. The decision to use other invasive assessments was at the discretion of the operator. This report describes an early series of the 14 patients who underwent FFR of 18 target stenoses in addition to FD-OCT. FD-OCT was successfully performed without complications in all cases. Fractional flow reserve was <0.80 in four patients, with minimal lumen areas and reference vessel diameters ranging from 1.03 to 3.47 mm(2) and 2.60 to 2.94 mm by FD-OCT, respectively. FD-OCT was important to rule out plaque rupture, erosion and thrombosis and to help guide decision to defer PCI in six patients with acute coronary syndrome and FFR > 0.80. FD-OCT was also valuable to guide PCI strategy in tandem lesions with an FFR < 0.80. This initial experience with FD-OCT suggests a potential complementary role of physiological and anatomical assessment to guide decision making in complex clinical scenarios. Future investigations are warranted to validate these findings and define the role of FD-OCT in assessing intermediate lesions.
Figures
Similar articles
-
Evaluation of hemodynamically severe coronary stenosis as determined by fractional flow reserve with frequency domain optical coherence tomography measured anatomical parameters.J Cardiol. 2014 Jul;64(1):19-24. doi: 10.1016/j.jjcc.2013.11.009. Epub 2013 Dec 22. J Cardiol. 2014. PMID: 24368093
-
Feasibility of intracoronary frequency domain optical coherence tomography derived fractional flow reserve for the assessment of coronary artery stenosis.Int Heart J. 2014;55(4):307-11. doi: 10.1536/ihj.13-362. Epub 2014 Jun 6. Int Heart J. 2014. PMID: 24909988
-
Combined optical coherence tomography morphologic and fractional flow reserve hemodynamic assessment of non- culprit lesions to better predict adverse event outcomes in diabetes mellitus patients: COMBINE (OCT-FFR) prospective study. Rationale and design.Cardiovasc Diabetol. 2016 Oct 10;15(1):144. doi: 10.1186/s12933-016-0464-8. Cardiovasc Diabetol. 2016. PMID: 27724869 Free PMC article.
-
Diagnostic performance of fractional flow reserve derived from coronary angiography, intravascular ultrasound, and optical coherence tomography; a meta-analysis.J Cardiol. 2022 Jul;80(1):1-8. doi: 10.1016/j.jjcc.2022.02.015. Epub 2022 Mar 10. J Cardiol. 2022. PMID: 35282944
-
Optical coherence tomography enables more accurate detection of functionally significant intermediate non-left main coronary artery stenoses than intravascular ultrasound: A meta-analysis of 6919 patients and 7537 lesions.Int J Cardiol. 2020 Feb 15;301:226-234. doi: 10.1016/j.ijcard.2019.09.067. Epub 2019 Oct 9. Int J Cardiol. 2020. PMID: 31677827
Cited by
-
Optical Coherence Tomography: Potential Clinical Applications.Curr Cardiovasc Imaging Rep. 2012 Aug;5(4):206-220. doi: 10.1007/s12410-012-9140-x. Epub 2012 May 3. Curr Cardiovasc Imaging Rep. 2012. PMID: 22798978 Free PMC article.
-
Cardiovascular imaging 2011 in the International Journal of Cardiovascular Imaging.Int J Cardiovasc Imaging. 2012 Mar;28(3):439-51. doi: 10.1007/s10554-012-0040-6. Int J Cardiovasc Imaging. 2012. PMID: 22476909 Free PMC article. Review. No abstract available.
-
Optical coherence tomography imaging during percutaneous coronary intervention impacts physician decision-making: ILUMIEN I study.Eur Heart J. 2015 Dec 14;36(47):3346-55. doi: 10.1093/eurheartj/ehv367. Epub 2015 Aug 4. Eur Heart J. 2015. PMID: 26242713 Free PMC article.
-
Measurement of the blood flow rate and velocity in coronary artery stenosis using intracoronary frequency domain optical coherence tomography: Validation against fractional flow reserve.Int J Cardiol Heart Vasc. 2014 Oct 16;5:68-71. doi: 10.1016/j.ijcha.2014.10.004. eCollection 2014 Dec. Int J Cardiol Heart Vasc. 2014. PMID: 28785616 Free PMC article.
-
Fractional flow reserve or optical coherence tomography guidance to revascularize intermediate coronary stenosis using angioplasty (FORZA) trial: study protocol for a randomized controlled trial.Trials. 2014 Apr 23;15:140. doi: 10.1186/1745-6215-15-140. Trials. 2014. PMID: 24758510 Free PMC article. Clinical Trial.
References
-
- Pijls NH, van Schaardenburgh P, Manoharan G, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER study. J Am Coll Cardiol. 2007;49:2105–2111. - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, on behalf of FAME Study Investigators et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–224. - PubMed
-
- Costa MA, Sabate M, Staico R, et al. Anatomical and physiologic assessments in patients with small coronary artery disease: final results of the physiologic and anatomical evaluation prior to and after stent implantation in small coronary vessels (PHANTOM) trial. Am Heart J. 2007;153:296.e1–7. - PubMed
-
- Abizaid AS, Mintz GS, Mehran R, et al. Long-term follow-up after percutaneous transluminal coronary angioplasty was not performed based on intravascular ultra-sound findings: Importance of lumen dimensions. Circulation. 1999;100:256–261. - PubMed
-
- Briguori C, Anzuini A, Airoldi F, et al. Intravascular ultrasound criteria for the assessment of the functional significance of intermediate coronary artery stenoses and comparison with fractional flow reserve. Am J Cardiol. 2001;87:136–141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
