

The cost of providing comprehensive HIV treatment in PEPFAR-supported programs
- PMID: 21412127
- PMCID: PMC3225224
- DOI: 10.1097/QAD.0b013e3283463eec
The cost of providing comprehensive HIV treatment in PEPFAR-supported programs
Abstract
Background: PEPFAR, national governments, and other stakeholders are investing unprecedented resources to provide HIV treatment in developing countries. This study reports empirical data on costs and cost trends in a large sample of HIV treatment sites.
Design: In 2006-2007, we conducted cost analyses at 43 PEPFAR-supported outpatient clinics providing free comprehensive HIV treatment in Botswana, Ethiopia, Nigeria, Uganda, and Vietnam.
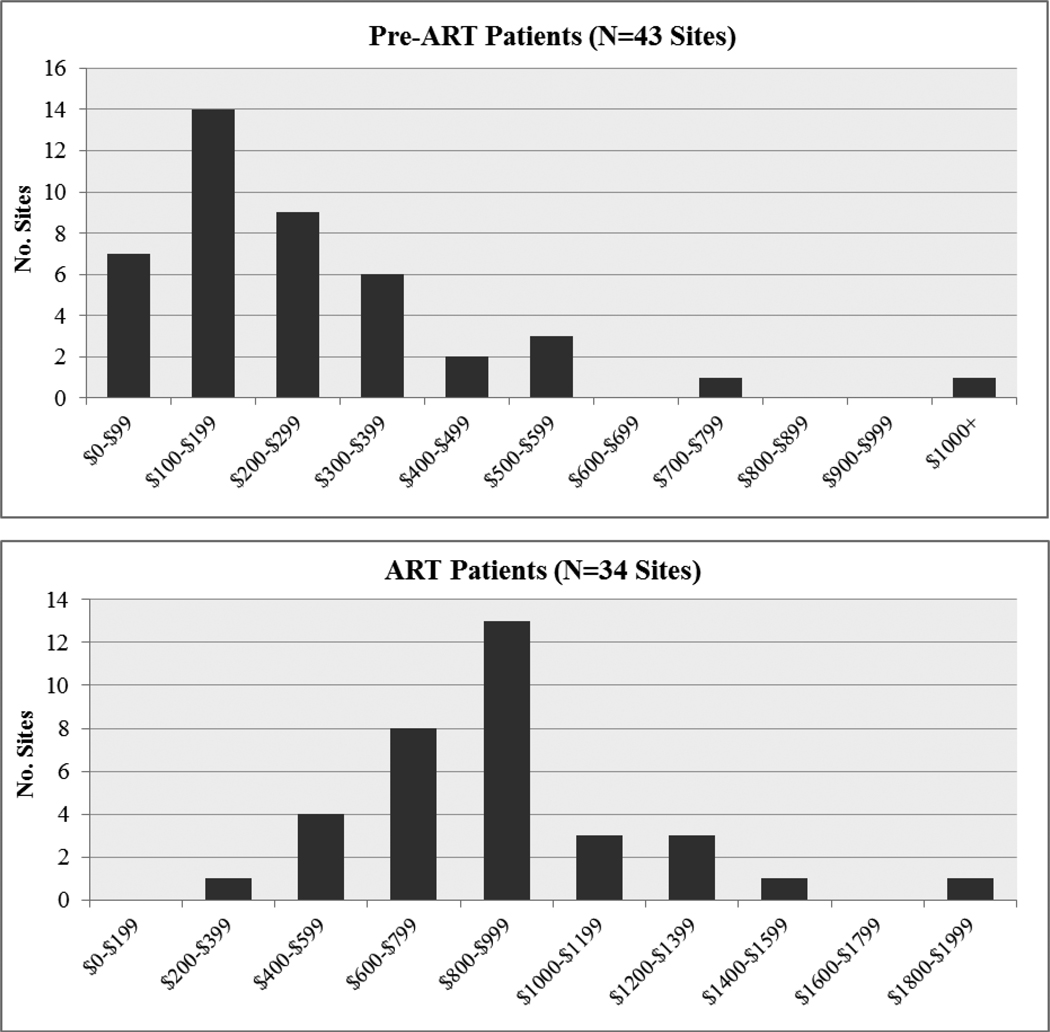
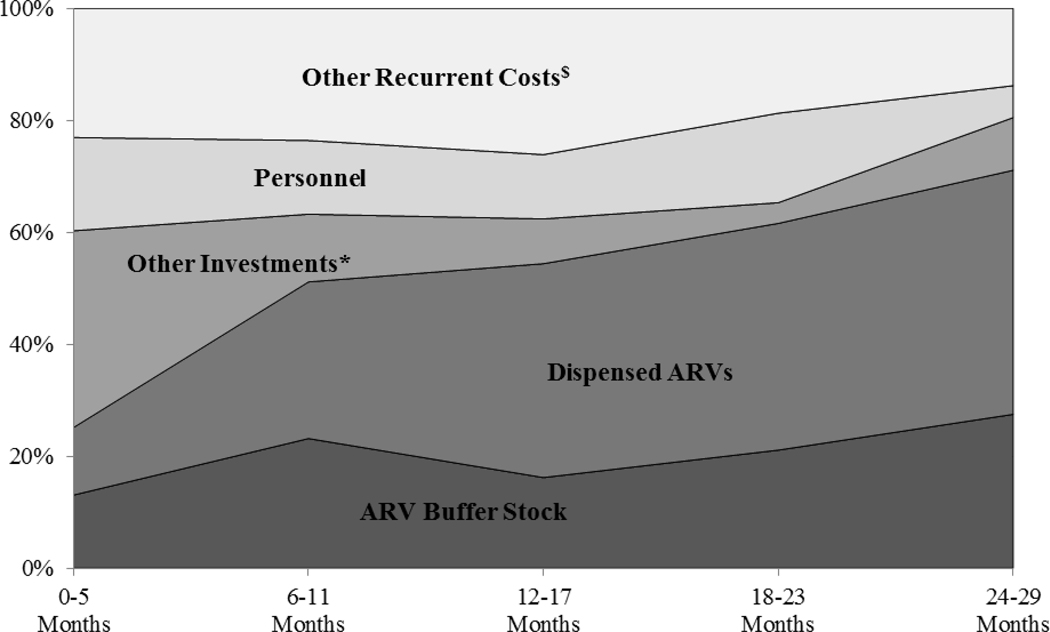
Methods: We collected data on HIV treatment costs over consecutive 6-month periods starting from scale-up of dedicated HIV treatment services at each site. The study included all patients receiving HIV treatment and care at study sites [62,512 antiretroviral therapy (ART) and 44,394 pre-ART patients]. Outcomes were costs per patient and total program costs, subdivided by major cost categories.
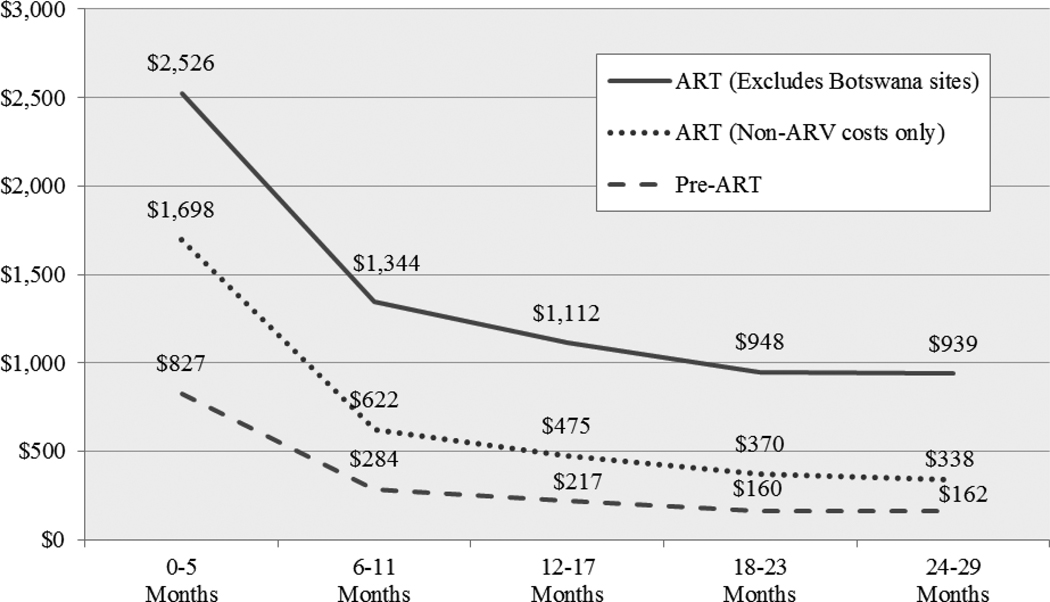
Results: Median annual economic costs were US$ 202 (2009 USD) for pre-ART patients and US$ 880 for ART patients. Excluding antiretrovirals, per patient ART costs were US$ 298. Care for newly initiated ART patients cost 15-20% more than for established patients. Per patient costs dropped rapidly as sites matured, with per patient ART costs dropping 46.8% between first and second 6-month periods after the beginning of scale-up, and an additional 29.5% the following year. PEPFAR provided 79.4% of funding for service delivery, and national governments provided 15.2%.
Conclusion: Treatment costs vary widely between sites, and high early costs drop rapidly as sites mature. Treatment costs vary between countries and respond to changes in antiretroviral regimen costs and the package of services. Whereas cost reductions may allow near-term program growth, programs need to weigh the trade-off between improving services for current patients and expanding coverage to new patients.
Figures
Comment in
-
Can cost studies improve the performance of donor-financed HIV treatment?AIDS. 2011 Sep 10;25(14):1795-6. doi: 10.1097/QAD.0b013e32834a1f77. AIDS. 2011. PMID: 21785322 No abstract available.
References
-
- UNAIDS. What countries need: investments needed for 2010 targets. Geneva: UNAIDS; 2009.
-
- UNAIDS. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector: progress report 2009. Geneva: UNAIDS; 2009.
-
- United Nations. Political declaration on HIV/AIDS: resolution adopted by the General Assembly 60/262. New York: United Nations General Assembly; 2006.
-
- Cleary SM, McIntyre D, Boulle AM. Assessing efficiency and costs of scaling up HIV treatment. AIDS. 2008;22 Suppl 1:S35–S42. - PubMed
-
- Quentin W, Konig H-H, Schmidt J-O, Kalk A. Recurrent costs of HIV/AIDS-related health services in Rwanda: implications for financing. Trop Med Int Health. 2008;13(10):1245–1256. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
