

A multidisciplinary approach to transition care: a patient safety innovation study
- PMID: 21412475
- PMCID: PMC3048437
- DOI: 10.7812/TPP/07-012
A multidisciplinary approach to transition care: a patient safety innovation study
Abstract
Introduction: Patients with complex medical care needs often embark on multiple care transitions over an extended period of time. As these patients or their caregivers often become the chief source of communication for complex medical situations, each transition can create an opportunity for health care errors. Combining the efforts of the established departments of Chronic Care Coordination (CCC), Clinical Pharmacy Call Center (CPCC), and Continuing Care, Kaiser Permanente Colorado created programs to further safe care transitions.
Methods: Two key goals for safe care transitions were established: 1) reductions in medication errors and 2) increased follow-up with care plans. To achieve these goals, communication plans targeted at medication reconciliation, patient education, and coordination of outpatient recommendations were established. Expected outcomes included reductions in medication errors, decreased Emergency Department and hospital admissions, decreased readmissions, and increased outpatient follow-up and medication compliance.
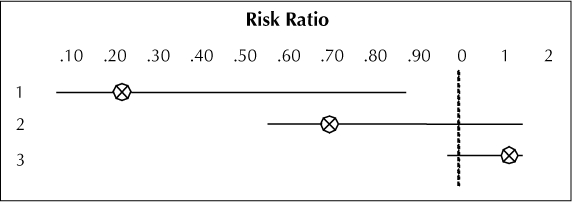
Results: A review of medication-reconciliation records for intervention patients indicated that >90% of all discharge summaries contained at least one potential drug-related problem including duplicative drugs, omitted therapy, and medication contraindications. After skilled nursing facility discharge, patients who were transitioned by CPCC clinical pharmacists were: 1) 78% less likely to die; 2) 29% less likely to need an Emergency Department visit; and 3) 17% more likely to follow up with primary physicians and clinicians than were patients in the usual care group. Health care cost savings for patients seen by the CCC program demonstrated, conservatively, an annualized per patient savings of $5276. For 763 patients enrolled in 2003, this amounts to an estimated, annualized savings of $4,025,588.
Conclusions: Patients are becoming more informed and involved in their care, but they require ongoing education and coaching to become effective advocates for themselves. Identification of unintended medication discrepancies and potential drug-related problems and increased follow-up during care transitions can improve patient safety and quality of care while saving health care resources.
Figures
Similar articles
-
Florida Controlled Substance Prescribing.2022 Oct 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2022 Oct 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33428370 Free Books & Documents.
-
Clinical outcomes of a home-based medication reconciliation program after discharge from a skilled nursing facility.Pharmacotherapy. 2008 Apr;28(4):444-52. doi: 10.1592/phco.28.4.444. Pharmacotherapy. 2008. PMID: 18363528 Clinical Trial.
-
NP Safe Prescribing of Controlled Substances While Avoiding Drug Diversion.2023 Jan 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Jan 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33232099 Free Books & Documents.
-
Evidence Brief: The Quality of Care Provided by Advanced Practice Nurses [Internet].Washington (DC): Department of Veterans Affairs (US); 2014 Sep. Washington (DC): Department of Veterans Affairs (US); 2014 Sep. PMID: 27606392 Free Books & Documents. Review.
-
Evidence Brief: Effectiveness of Intensive Primary Care Programs [Internet].Washington (DC): Department of Veterans Affairs (US); 2013 Feb. Washington (DC): Department of Veterans Affairs (US); 2013 Feb. PMID: 27606397 Free Books & Documents. Review.
Cited by
-
How health systems facilitate patient-centered care and care coordination: a case series analysis to identify best practices.BMC Health Serv Res. 2022 Nov 29;22(1):1448. doi: 10.1186/s12913-022-08623-w. BMC Health Serv Res. 2022. PMID: 36447273 Free PMC article. Review.
-
The Impact of an Infectious Diseases Transition Service on the Care of Outpatients on Parenteral Antimicrobial Therapy.J Pharm Technol. 2013 Oct;29(5):205-214. doi: 10.1177/8755122513500922. J Pharm Technol. 2013. PMID: 25621307 Free PMC article.
-
The effect of clinical interventions on hospital readmissions: a meta-review of published meta-analyses.Isr J Health Policy Res. 2013 Jan 23;2(1):1. doi: 10.1186/2045-4015-2-1. Isr J Health Policy Res. 2013. PMID: 23343012 Free PMC article.
-
Perceived Self-Efficacy, Confidence, and Skill Among Factors of Adult Patient Participation in Transitional Care: A Systematic Review of Quantitative Studies.SAGE Open Nurs. 2022 Jan 28;8:23779608221074658. doi: 10.1177/23779608221074658. eCollection 2022 Jan-Dec. SAGE Open Nurs. 2022. PMID: 35111928 Free PMC article. Review.
-
Community Pharmacists' Experiences and Perception about Transitions of Care from Hospital to Home in a Midwestern Metropolis.Pharmacy (Basel). 2021 Nov 27;9(4):193. doi: 10.3390/pharmacy9040193. Pharmacy (Basel). 2021. PMID: 34941625 Free PMC article.
References
-
- Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003 Apr;51(4):549–55. - PubMed
-
- Parry C, Kramer HM, Coleman EA. A qualitative exploration of a patient-centered coaching intervention to improve care transitions in chronically ill older adults. Home Health Care Serv Q. 2006;25(3–4):39–53. - PubMed
-
- Siegler EL, Murtaugh CM, Rosati RJ et al. Improving the transition to home healthcare by rethinking the purpose and structure of the CMS 485: first steps. Health Care Serv Q. 2006;25(3–4):27–38. - PubMed
-
- Halasyamani L, Kripalani S, Coleman E et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354–60. - PubMed
-
- Coleman EA, Smith JD, Frank JC. Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention. J Am Geriatr Soc. 2004 Nov;52(100):1817–25. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
