

Management of stage IV rectal cancer: palliative options
- PMID: 21412493
- PMCID: PMC3051134
- DOI: 10.3748/wjg.v17.i7.835
Management of stage IV rectal cancer: palliative options
Abstract
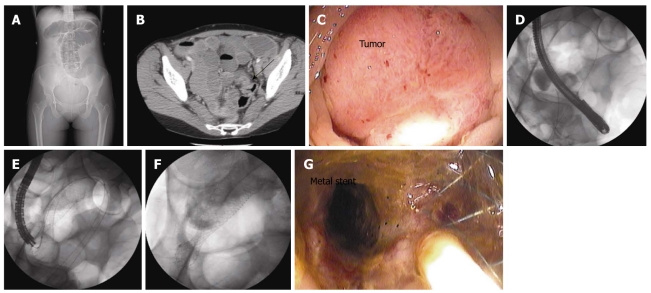
Approximately 30% of patients with rectal cancer present with metastatic disease. Many of these patients have symptoms of bleeding or obstruction. Several treatment options are available to deal with the various complications that may afflict these patients. Endorectal stenting, laser ablation, and operative resection are a few of the options available to the patient with a malignant large bowel obstruction. A thorough understanding of treatment options will ensure the patient is offered the most effective therapy with the least amount of associated morbidity. In this review, we describe various options for palliation of symptoms in patients with metastatic rectal cancer. Additionally, we briefly discuss treatment for asymptomatic patients with metastatic disease.
Keywords: Endorectal stenting; Laser ablation; Malignant bleeding; Malignant obstruction; Palliative therapy; Rectal cancer.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Rothenberger DA. Palliative therapy of rectal cancer. Overview: epidemiology, indications, goals, extent, and nature of work-up. J Gastrointest Surg. 2004;8:259–261. - PubMed
-
- Van Cutsem E, Oliveira J. Advanced colorectal cancer: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;20 Suppl 4:61–63. - PubMed
-
- Engstrom PF, Arnoletti JP, Benson AB 3rd, Chen YJ, Choti MA, Cooper HS, Covey A, Dilawari RA, Early DS, Enzinger PC, et al. NCCN Clinical Practice Guidelines in Oncology: rectal cancer. J Natl Compr Canc Netw. 2009;7:838–881. - PubMed
-
- Miner TJ, Jaques DP, Tavaf-Motamen H, Shriver CD. Decision making on surgical palliation based on patient outcome data. Am J Surg. 1999;177:150–154. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
