

Non-surgical interventions for convergence insufficiency
- PMID: 21412896
- PMCID: PMC4278667
- DOI: 10.1002/14651858.CD006768.pub2
Non-surgical interventions for convergence insufficiency
Update in
-
Interventions for convergence insufficiency: a network meta-analysis.Cochrane Database Syst Rev. 2020 Dec 2;12(12):CD006768. doi: 10.1002/14651858.CD006768.pub3. Cochrane Database Syst Rev. 2020. PMID: 33263359 Free PMC article.
Abstract
Background: Convergence insufficiency is a common eye muscle co-ordination problem in which the eyes have a strong tendency to drift outward (exophoria) when reading or doing close work. Symptoms may include eye strain, headaches, double vision, print moving on the page, frequent loss of place when reading, inability to concentrate, and short attention span.
Objectives: To systematically assess and synthesize evidence from randomized controlled trials (RCTs) on the effectiveness of non-surgical interventions for convergence insufficiency.
Search strategy: We searched The Cochrane Library, MEDLINE, EMBASE, Science Citation Index, the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com) and ClinicalTrials.gov (www.clinicaltrials.gov ) on 7 October 2010. We manually searched reference lists and optometric journals.
Selection criteria: We included RCTs examining any form of non-surgical intervention against placebo, no treatment, sham treatment, or each other.
Data collection and analysis: Two authors independently assessed eligibility, risk of bias, and extracted data. We performed meta-analyses when appropriate.
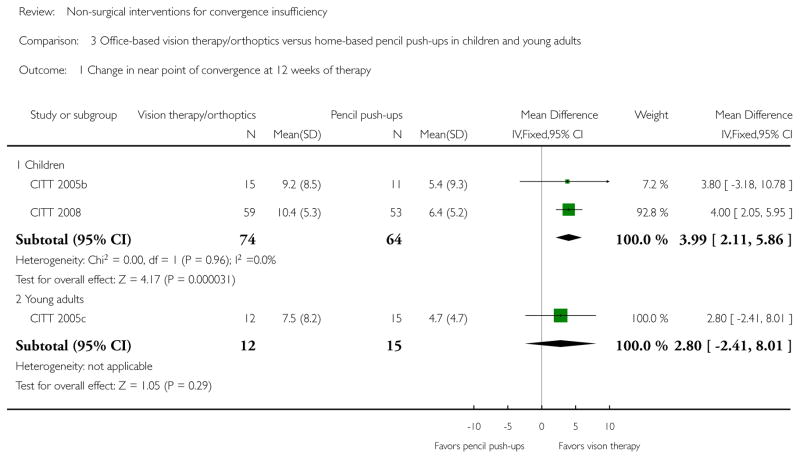
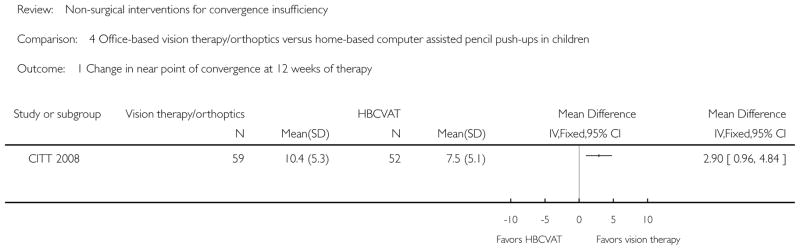
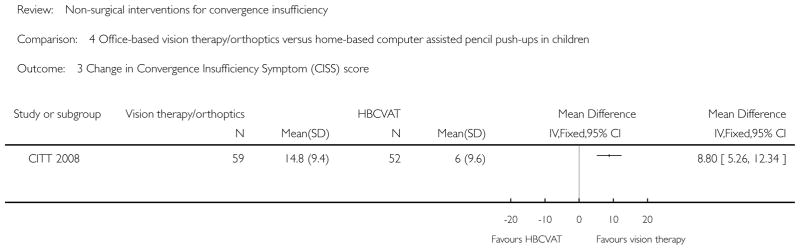
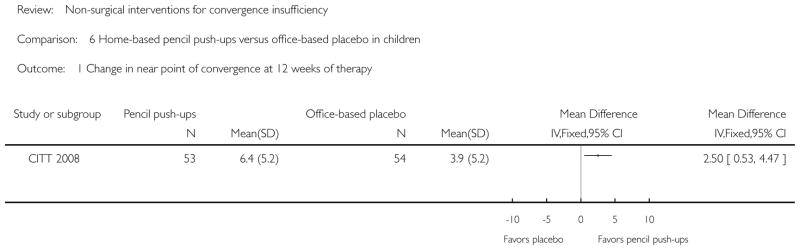
Main results: We included six trials (three in children, three in adults) with a total of 475 participants. We graded four trials at low risk of bias.Evidence from one trial (graded at low risk of bias) suggests that base-in prism reading glasses was no more effective than placebo reading glasses in improving clinical signs or symptoms in children.Evidence from one trial (graded at high risk of bias) suggests that base-in prism glasses using a progressive addition lens design was more effective than progressive addition lens alone in decreasing symptoms in adults. At three weeks of therapy, the mean difference in Convergence Insufficiency Symptoms Survey (CISS) score was -10.24 points (95% confidence interval (CI) -15.45 to -5.03).Evidence from two trials (graded at low risk of bias) suggests that outpatient (or office-based as used in the US) vision therapy/orthoptics was more effective than home-based convergence exercises (or pencil push-ups as used in the US) in children. At 12 weeks of therapy, the mean difference in change in near point of convergence, positive fusional vergence, and CISS score from baseline was 3.99 cm (95% CI 2.11 to 5.86), 13.13 diopters (95% CI 9.91 to 16.35), and 9.86 points (95% CI 6.70 to 13.02), respectively.In a young adult population, evidence from one trial (graded at low risk of bias) suggests outpatient vision therapy/orthoptics was more effective than home-based convergence exercises in improving positive fusional vergence at near (7.7 diopters, 95% CI 0.82 to 14.58), but not the other outcomes.Evidence from one trial (graded at low risk of bias) comparing four interventions, also suggests that outpatient vision therapy/orthoptics was more effective than home-based computer vision therapy/orthoptics in children. At 12 weeks, the mean difference in change in near point of convergence, positive fusional vergence, and CISS score from baseline was 2.90 cm (95% CI 0.96 to 4.84), 7.70 diopters (95% CI 3.94 to 11.46), and 8.80 points (95% CI 5.26 to 12.34), respectively. Evidence was less consistent for other pair-wise comparisons.
Authors' conclusions: Current research suggests that outpatient vision therapy/orthoptics is more effective than home-based convergence exercises or home-based computer vision therapy/orthoptics for children. In adult population, evidence of the effectiveness of various non-surgical interventions is less consistent.
Conflict of interest statement
Mitchell Scheiman, OD is the Study Chair of the Convergence Insufficiency Treatment Trial (CITT) Study Group. This group completed three of the clinical trials described in this paper and the group continues to investigate treatment of convergence insufficiency in children and adults.
Figures



















References
References to studies included in this review
-
- Birnbaum MH, Soden R, Cohen AH. Efficacy of vision therapy for convergence insufficiency in an adult male population. Journal of the American Optometric Association. 1999;70(4):225–32. - PubMed
-
- Scheiman M, Cotter S, Rouse M, Mitchell GL, Kulp M, Cooper J, et al. Convergence Insufficiency Treatment Trial Study Group. Randomised clinical trial of the effectiveness of base-in prism reading glasses versus placebo reading glasses for symptomatic convergence insufficiency in children. British Journal of Ophthalmology. 2005;89(10):1318–23. - PMC - PubMed
-
- Scheiman M, Mitchell GL, Cotter S, Cooper J, Kulp M, Rouse M, et al. Convergence Insufficiency Treatment Trial Study Group. A randomized clinical trial of treatments for convergence insufficiency in children. Archives of Ophthalmology. 2005;123(1):14–24. - PubMed
-
- Scheiman M, Mitchell GL, Cotter S, Kulp MT, Cooper J, Rouse M, et al. A randomized clinical trial of vision therapy/orthoptics versus pencil pushups for the treatment of convergence insufficiency in young adults. Optometry and Vision Science. 2005;82(7):583–95. - PubMed
-
- Convergence Insufficiency Treatment Trial (CITT) Study Group. The convergence insufficiency treatment trial: design, methods, and baseline data. Ophthalmic Epidemiology. 2008;15(1):24–36. - PMC - PubMed
- Convergence Insufficiency Treatment Trial Study Group. Long-term effectiveness of treatments for symptomatic convergence insufficiency in children. Optometry and Vision Science. 2009;86(9):1096–103. - PMC - PubMed
- Convergence Insufficiency Treatment Trial Study Group. Randomized clinical trial of treatments for symptomatic convergence insufficiency in children. Archives of Ophthalmology. 2008;126(10):1336–49. - PMC - PubMed
- Kulp M, Mitchell GL, Borsting E, Scheiman M, Cotter S, Rouse M, et al. Convergence Insufficiency Treatment Trial Study Group. Effectiveness of placebo therapy for maintaining masking in a clinical trial of vergence/accommodative therapy. Investigative Ophthalmology & Vision Science. 2009;50(6):2560–6. - PMC - PubMed
References to studies excluded from this review
-
- al-Qurainy IA. Convergence insufficiency and failure of accommodation following midfacial trauma. British Journal of Oral and Maxillofacial Surgery. 1995;33(2):71–5. - PubMed
-
- Daum KM. Characteristics of exodeviations: II. Changes with treatment with orthoptics. American Journal of Optometry and Physiological Optics. 1986;63(4):244–51. - PubMed
-
- Daum KM, Rutstein RP, Eskridge JB. Efficacy of computerized vergence therapy. American Journal of Optometry and Physiological Optics. 1987;64(2):83–9. - PubMed
-
- Dragomir M, Tru L, Chiril D, Stingu C. Orthoptic treatment efficiency in convergence insufficiency treatment. Oftalmologia. 2001;53(3):66–9. - PubMed
-
- Frantz KA, Cotter SA, Scharre JE, Coffey B, Harrist R, Horner D, et al. Pilot study of a vision therapy protocol for intermittent exotropia. American Academy of Optometry. 1993:14.
Additional references
-
- Aikon DL. Memory traces in the brain. New York: Cambridge University Press; 1988.
-
- Arbib MA. Perceptual structures and distributed motor control. Handbook of physiology. Vol. II: Motor control. Bethesda, MD: Brooks BV. American Physiological Society; 1981.
-
- Beecher HK. The powerful placebo. Journal of the American Medical Association. 1955;159(17):1602–6. - PubMed
-
- Birnbaum MH. The role of the trainer in visual training. Journal of American Optometric Association. 1977;48(8):1035–9. - PubMed
-
- Borsting EJ, Rouse MW. Validity and reliability of the revised convergence insufficiency symptom survey in children ages 9–18 years. Optometry and Vision Science. 2003;80(12):832–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical