

Use of aspirin associates with longer primary patency of hemodialysis grafts
- PMID: 21415156
- PMCID: PMC3065232
- DOI: 10.1681/ASN.2010060582
Use of aspirin associates with longer primary patency of hemodialysis grafts
Abstract
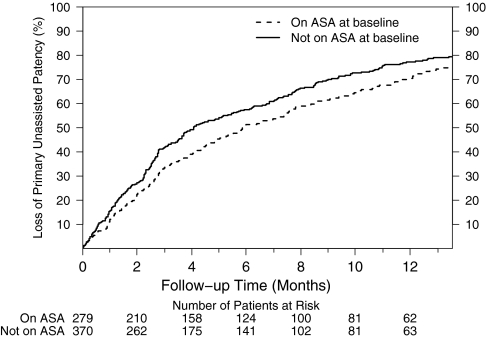
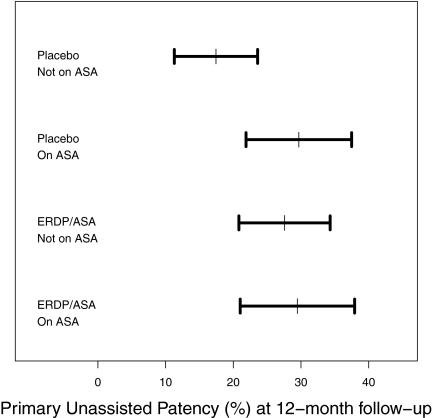
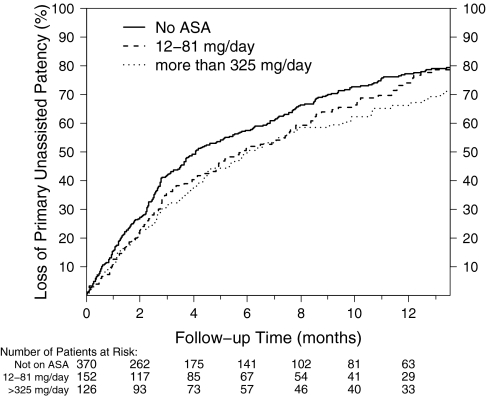
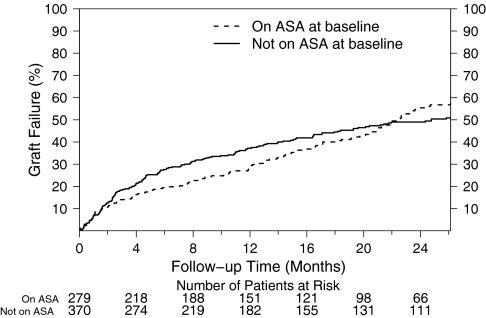
Extended-release dipyridamole plus low-dose aspirin (ERDP/ASA) prolongs primary unassisted graft patency of newly created hemodialysis arteriovenous grafts, but the individual contributions of each component are unknown. Here, we analyzed whether use of aspirin at baseline associated with primary unassisted graft patency among participants in a randomized trial that compared ERDP/ASA and placebo in newly created grafts. We used Cox proportional hazards regression, adjusting for prespecified baseline comorbidities and covariates. Of all participants, 43% reported use of aspirin at baseline; of these, 82% remained on nonstudy aspirin (i.e., excluding ERDP/ASA) at 1 year. After 1 year of follow-up, the incidence of primary unassisted patency among participants using aspirin at baseline was 30% (95% CI: 24 to 35%) and among those not using aspirin was 23% (95% CI: 18 to 27%). Use of aspirin at baseline associated with a dose-dependent prolongation of primary unassisted graft patency that approached statistical significance (adjusted HR, 0.83; 95% CI: 0.68 to 1.01; P=0.06). Use of aspirin at baseline did not associate with prolongation of cumulative graft patency or participant survival. In conclusion, use of aspirin associates with a trend toward longer primary unassisted patency of newly placed hemodialysis grafts similar to that observed for ERDP/ASA.
Copyright © 2011 by the American Society of Nephrology
Figures
Comment in
-
Aspirin and arteriovenous graft thrombosis in hemodialysis: just what the doctor ordered?J Am Soc Nephrol. 2011 Apr;22(4):595-7. doi: 10.1681/ASN.2011020181. Epub 2011 Mar 17. J Am Soc Nephrol. 2011. PMID: 21415154 No abstract available.
References
-
- Feldman HI, Kobrin S, Wasserstein A: Hemodialysis vascular access morbidity. J Am Soc Nephrol 7: 523–535, 1996 - PubMed
-
- Besarab A, Work J: Clinical practice guidelines for vascular access. Am J Kidney Dis 48[Suppl 1]: S176–S247, 2006 - PubMed
-
- Gibson KD, Gillen DL, Caps MT, Kohler TR, Sherrard DJ, Stehman-Breen CO: Vascular access survival and incidence of revisions: a comparison of prosthetic grafts, simple autogenous fistulas, and venous transposition fistulas from the United States Renal Data System Dialysis Morbidity and Mortality Study. J Vasc Surg 34: 694–700, 2001 - PubMed
-
- U.S. Renal Data System: 2008 Annual Data Report: Atlas of End-stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD: 2008
-
- Kanterman RY, Vesely TM, Pilgram TK, Guy BW, Windus DW, Picus D: Dialysis access grafts: Anatomic location of venous stenosis and results of angioplasty. Radiology 195: 135–139, 1995 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK058982/DK/NIDDK NIH HHS/United States
- U01 DK058986/DK/NIDDK NIH HHS/United States
- U01DK058978/DK/NIDDK NIH HHS/United States
- U01DK058985/DK/NIDDK NIH HHS/United States
- U01DK058986/DK/NIDDK NIH HHS/United States
- U01 DK058973/DK/NIDDK NIH HHS/United States
- U01DK058966/DK/NIDDK NIH HHS/United States
- U01 DK058966/DK/NIDDK NIH HHS/United States
- U01 DK058981/DK/NIDDK NIH HHS/United States
- U01DK058982/DK/NIDDK NIH HHS/United States
- U01 DK058968/DK/NIDDK NIH HHS/United States
- U01DK058973/DK/NIDDK NIH HHS/United States
- U01 DK058978/DK/NIDDK NIH HHS/United States
- U01DK058981/DK/NIDDK NIH HHS/United States
- U01 DK058985/DK/NIDDK NIH HHS/United States
- U01DK058968/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
