

Clinical utility of genetic testing in children and adults with steroid-resistant nephrotic syndrome
- PMID: 21415313
- PMCID: PMC3087781
- DOI: 10.2215/CJN.05260610
Clinical utility of genetic testing in children and adults with steroid-resistant nephrotic syndrome
Abstract
Background and objectives: The increasing number of podocyte-expressed genes implicated in steroid-resistant nephrotic syndrome (SRNS), the phenotypic variability, and the uncharacterized relative frequency of mutations in these genes in pediatric and adult patients with SRNS complicate their routine genetic analysis. Our aim was to compile the clinical and genetic data of eight podocyte genes analyzed in 110 cases (125 patients) with SRNS (ranging from congenital to adult onset) to provide a genetic testing approach.
Design, setting, participants, & measurements: Mutation analysis was performed by sequencing the NPHS1, NPHS2, TRPC6, CD2AP, PLCE1, INF2, WT1 (exons 8 and 9), and ACTN4 (exons 1 to 10) genes.
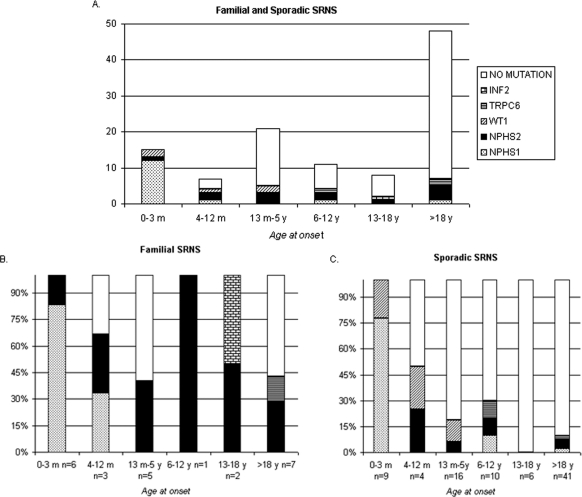
Results: We identified causing mutations in 34% (37/110) of SRNS patients, representing 67% (16/24) familial and 25% (21/86) sporadic cases. Mutations were detected in 100% of congenital-onset, 57% of infantile-onset, 24 and 36% of early and late childhood-onset, 25% of adolescent-onset, and 14% of adult-onset patients. The most frequently mutated gene was NPHS1 in congenital onset and NPHS2 in the other groups. A partial remission was observed in 7 of 26 mutation carriers treated with immunosuppressive agents and/or angiotensin-converting enzyme inhibitors. Patients with NPHS1 mutations showed a faster progression to ESRD than patients with NPHS2 mutations. None of these mutation carriers relapsed after kidney transplantation.
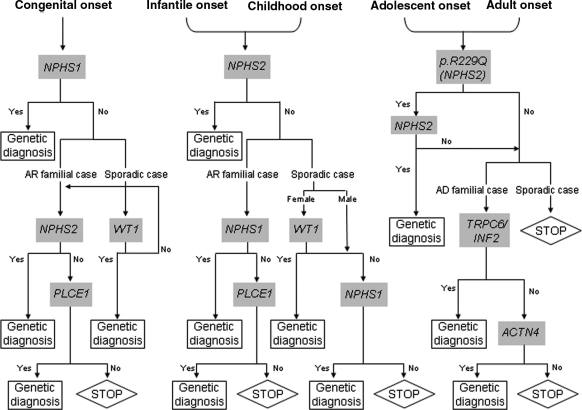
Conclusions: We propose a genetic testing algorithm for SRNS based on the age at onset and the familial/sporadic status. Mutation analysis of specific podocyte-genes has a clinical value in all age groups, especially in children.
Copyright © 2011 by the American Society of Nephrology
Figures
References
-
- Short versus standard prednisone therapy for initial treatment of idiopathic nephrotic syndrome in children. Arbeitsgemeinschaft fur Padiatrische Nephrologie. Lancet 1: 380–383, 1988 - PubMed
-
- Tune BM, Mendoza SA: Treatment of the idiopathic nephrotic syndrome: Regimens and outcomes in children and adults. J Am Soc Nephrol 8: 824–832, 1997 - PubMed
-
- Braden GL, Mulhern JG, O'Shea MH, Nash SV, Ucci AA, Jr, Germain MJ: Changing incidence of glomerular diseases in adults. Am J Kidney Dis 35: 878–883, 2000 - PubMed
-
- Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC: Focal and segmental glomerulosclerosis: Definition and relevance of a partial remission. J Am Soc Nephrol 16: 1061–1068, 2005 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
