

Cardiac myosin activation: a potential therapeutic approach for systolic heart failure
- PMID: 21415352
- PMCID: PMC4090309
- DOI: 10.1126/science.1200113
Cardiac myosin activation: a potential therapeutic approach for systolic heart failure
Abstract
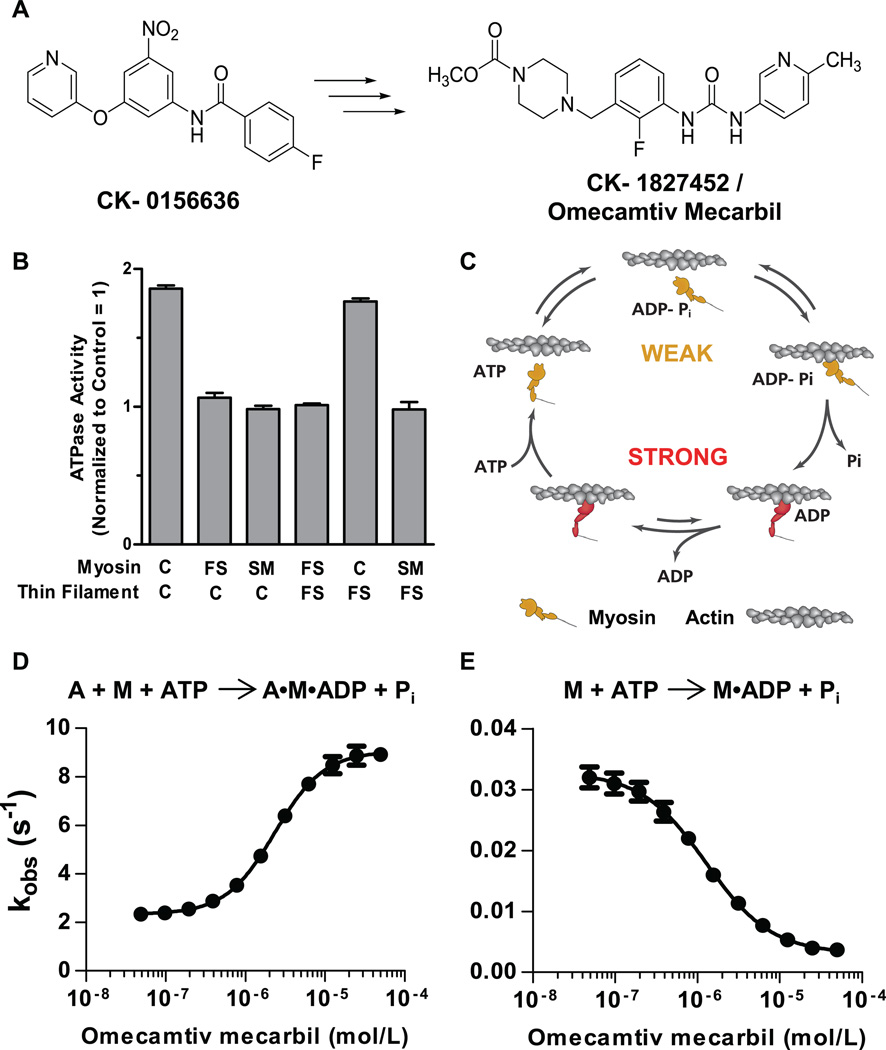
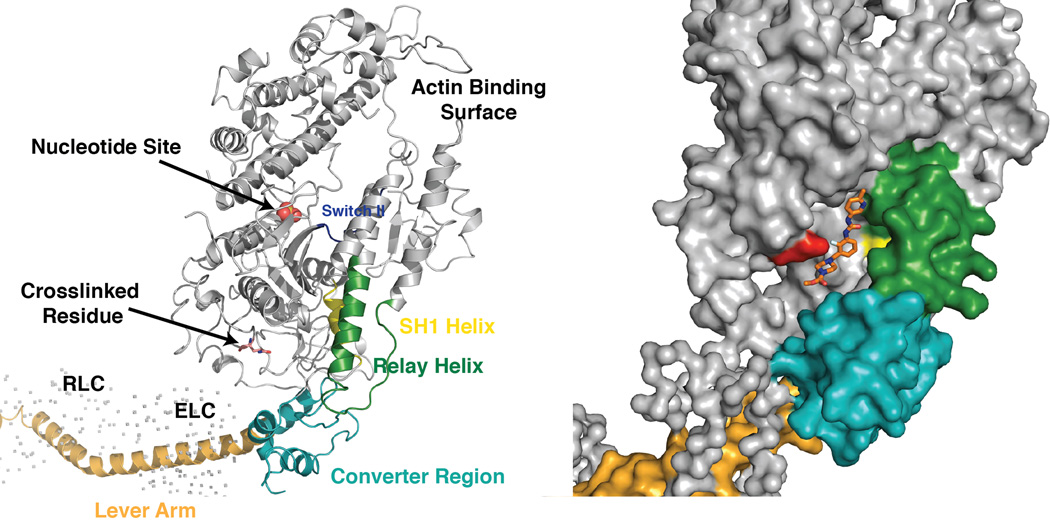
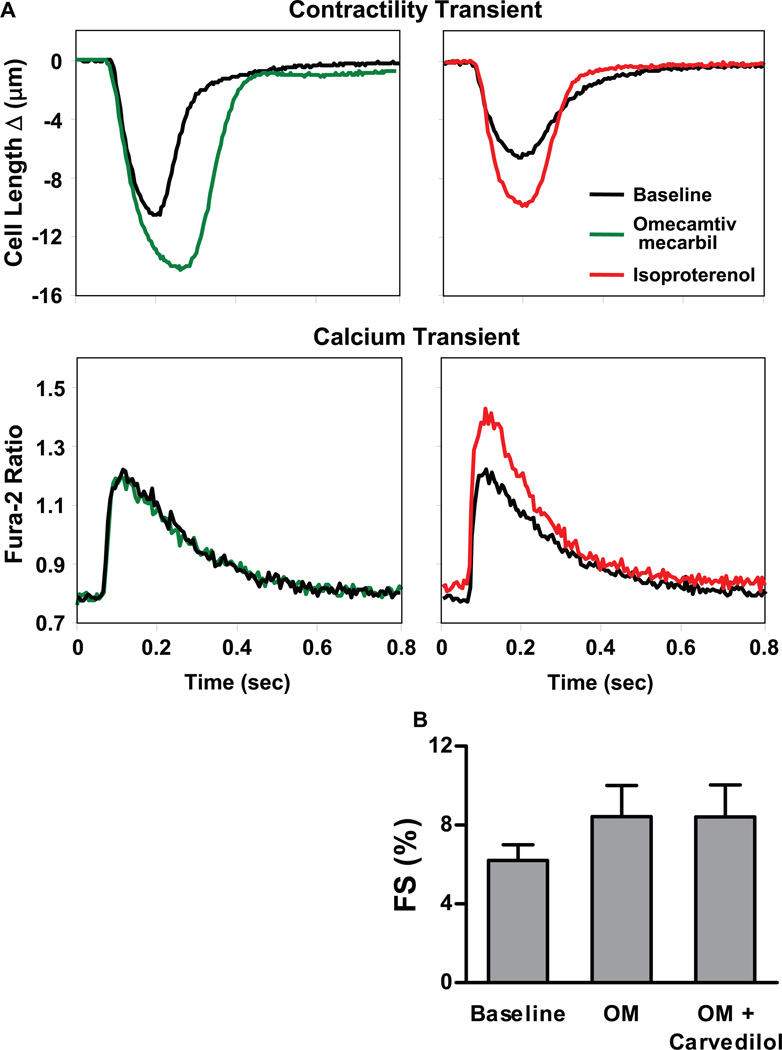
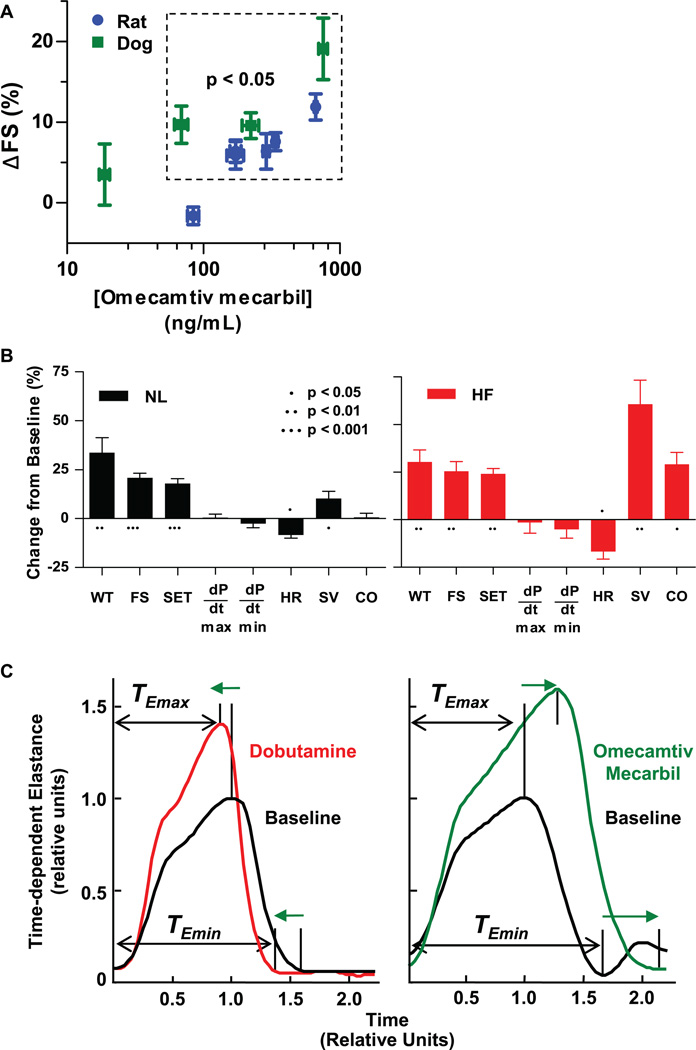
Decreased cardiac contractility is a central feature of systolic heart failure. Existing drugs increase cardiac contractility indirectly through signaling cascades but are limited by their mechanism-related adverse effects. To avoid these limitations, we previously developed omecamtiv mecarbil, a small-molecule, direct activator of cardiac myosin. Here, we show that it binds to the myosin catalytic domain and operates by an allosteric mechanism to increase the transition rate of myosin into the strongly actin-bound force-generating state. Paradoxically, it inhibits adenosine 5'-triphosphate turnover in the absence of actin, which suggests that it stabilizes an actin-bound conformation of myosin. In animal models, omecamtiv mecarbil increases cardiac function by increasing the duration of ejection without changing the rates of contraction. Cardiac myosin activation may provide a new therapeutic approach for systolic heart failure.
Figures
Comment in
-
Medicine. Chemically tuned myosin motors.Science. 2011 Mar 18;331(6023):1392-3. doi: 10.1126/science.1204207. Science. 2011. PMID: 21415340 No abstract available.
-
Cardiovascular disease: Powering up a failing heart.Nat Rev Drug Discov. 2011 May;10(5):338. doi: 10.1038/nrd3447. Nat Rev Drug Discov. 2011. PMID: 21532560 No abstract available.
-
At the source: treating heart failure by altering muscle motor function.Circ Res. 2011 Jun 24;109(1):5-7. doi: 10.1161/RES.0b013e31822765e2. Circ Res. 2011. PMID: 21700949 No abstract available.
References
-
- Lloyd-Jones D, et al. Executive summary: Heart disease and stroke statistics—2010 update: A report from the American Heart Association. Circulation. 2010;121:948. - PubMed
-
- Loehr LR, Rosamond WD, Chang PP, Folsom AR, Chambless LE. Heart failure incidence and survival (from the Atherosclerosis Risk in Communities study) Am. J. Cardiol. 2008;101:1016. - PubMed
-
- Adams KF, Jr, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE) Am. Heart J. 2005;149:209. - PubMed
-
- McMurray JJV. Clinical practice. Systolic heart failure. N. Engl. J. Med. 2010;362:228. - PubMed
-
- Kass DA, Solaro RJ. Mechanisms and use of calcium-sensitizing agents in the failing heart. Circulation. 2006;113:305. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
