

Hypothermic treatment for acute spinal cord injury
- PMID: 21416406
- PMCID: PMC3101829
- DOI: 10.1007/s13311-011-0035-3
Hypothermic treatment for acute spinal cord injury
Abstract
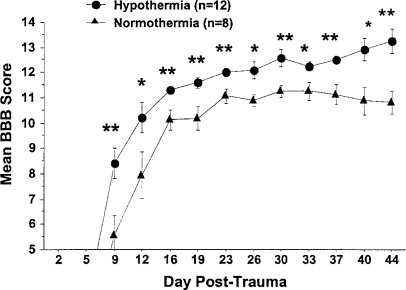
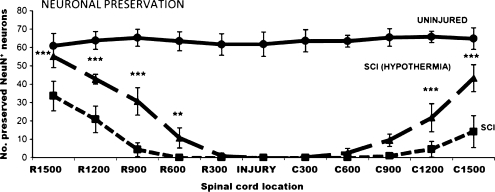
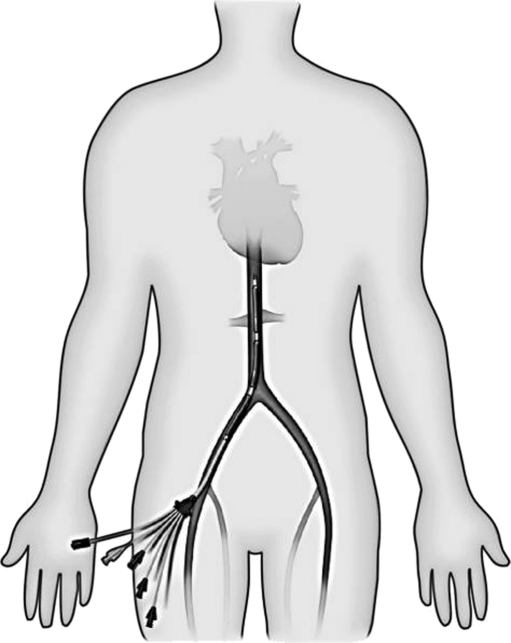
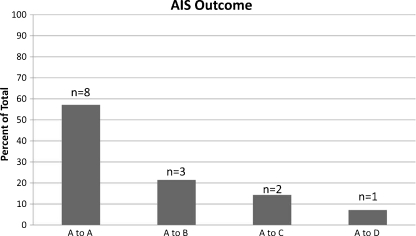
Spinal cord injury (SCI) is a devastating condition that affects approximately 11,000 patients each year in the United States. Although a significant amount of research has been conducted to clarify the pathophysiology of SCI, there are limited therapeutic interventions that are currently available in the clinic. Moderate hypothermia has been used in a variety of experimental and clinical situations to target several neurological disorders, including traumatic brain and SCI. Recent studies using clinically relevant animal models of SCI have reported the efficacy of therapeutic hypothermia (TH) in terms of promoting long-term behavioral improvement and reducing histopathological damage. In addition, several clinical studies have demonstrated encouraging evidence for the use of TH in patients with a severe cervical spinal cord injury. Moderate hypothermia (33°C) introduced systemically by intravascular cooling strategies appears to be safe and provides some improvement of long-term recovery of function. TH remains an experimental clinical approach and randomized multicenter trials are needed to critically evaluate this potentially exciting therapeutic intervention targeting this patient population.
Figures

References
-
- Spinal Cord Injury Facts and Figures at a Glance. University of Alabama, Birmingham, Alabama: National Spinal Cord Injury Statistical Center; 2010. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
