

Persistent organ dysfunction plus death: a novel, composite outcome measure for critical care trials
- PMID: 21418560
- PMCID: PMC3219367
- DOI: 10.1186/cc10110
Persistent organ dysfunction plus death: a novel, composite outcome measure for critical care trials
Abstract
Introduction: Due to resource limitations, few critical care interventions have been rigorously evaluated with adequately powered randomized clinical trials (RCTs). There is a need to improve the efficiency of RCTs in critical care so that more definitive high quality RCTs can be completed with the available resources. The objective of this study was to validate and demonstrate the utility of a novel composite outcome measure, persistent organ dysfunction (POD) plus death, for clinical trials of critically ill patients.
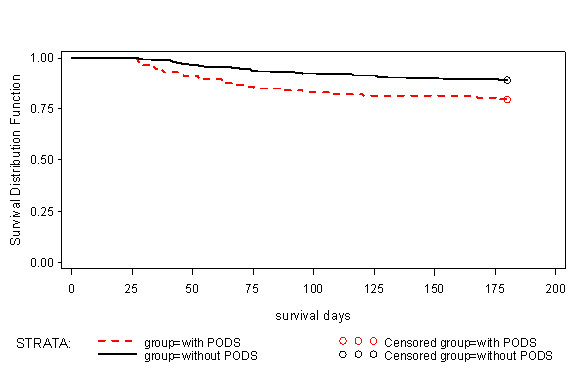
Methods: We performed a secondary analysis of a dataset from a prospective randomized trial involving 38 intensive care units (ICUs) in Canada, Europe, and the United States. We define POD as the persistence of organ dysfunction requiring supportive technologies during the convalescent phase of critical illness and it is present when a patient has an ongoing requirement for vasopressors, dialysis, or mechanical ventilation at the outcome assessments time points. In 600 patients enrolled in a randomized trial of nutrition therapy and followed prospectively for six months, we evaluated the prevalence of POD and its association with outcome.
Results: At 28 days, 2.3% of patients had circulatory failure, 13.7% had renal failure, 8.7% had respiratory failure, and 27.2% had died, for an overall prevalence of POD + death = 46.0%. Of survivors at Day 28, those with POD, compared to those without POD, had a higher mortality rate in the six-month follow-up period, had longer ICU and hospital stays, and a reduced quality of life at three months. Given these rates of POD + death and using a two-sided Chi-squared test at alpha = 0.05, we would require 616 patients per arm to detect a 25% relative risk reduction (RRR) in mortality, but only 286 per arm to detect the same RRR in POD + mortality.
Conclusions: POD + death may be a valid composite outcome measure and compared to mortality endpoints, may reduce the sample size requirements of clinical trials of critically ill patients. Further validation in larger clinical trials is required.
Figures
References
-
- Cohen J, Guyatt G, Bernard GR, Calandra T, Cook D, Elbourne D, Marshall J, Nunn A, Opal S. UK Medical Research Council International Working Party. New strategies for clinical trials in patients with sepsis and septic shock. Crit Care Med. 2001;29:880–886. doi: 10.1097/00003246-200104000-00039. - DOI - PubMed
-
- Vincent JL, Mendonca A, Cantraine F, Moreno R, Takala J, Suter P, Sprung CL, Colardyn F, Blecher S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Crit Care Med. 1998;26:1793–1800. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
