

Programmed death-1 levels correlate with increased mortality, nosocomial infection and immune dysfunctions in septic shock patients
- PMID: 21418617
- PMCID: PMC3219369
- DOI: 10.1186/cc10112
Programmed death-1 levels correlate with increased mortality, nosocomial infection and immune dysfunctions in septic shock patients
Abstract
Introduction: Septic shock remains a major health care problem worldwide. Sepsis-induced immune alterations are thought to play a major role in patients' mortality and susceptibility to nosocomial infections. Programmed death-1 (PD-1) receptor system constitutes a newly described immunoregulatory pathway that negatively controls immune responses. It has recently been shown that PD-1 knock-out mice exhibited a lower mortality in response to experimental sepsis. The objective of the present study was to investigate PD-1-related molecule expressions in septic shock patients.
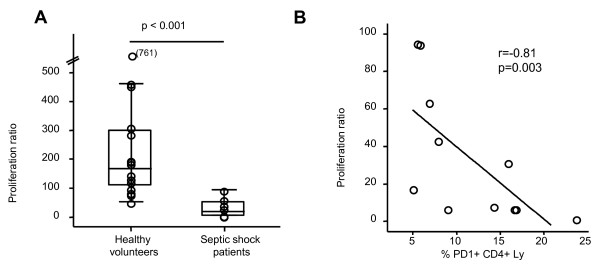
Methods: This prospective and observational study included 64 septic shock patients, 13 trauma patients and 49 healthy individuals. PD-1-related-molecule expressions were measured by flow cytometry on circulating leukocytes. Plasmatic interleukin (IL)-10 concentration as well as ex vivo mitogen-induced lymphocyte proliferation were assessed.
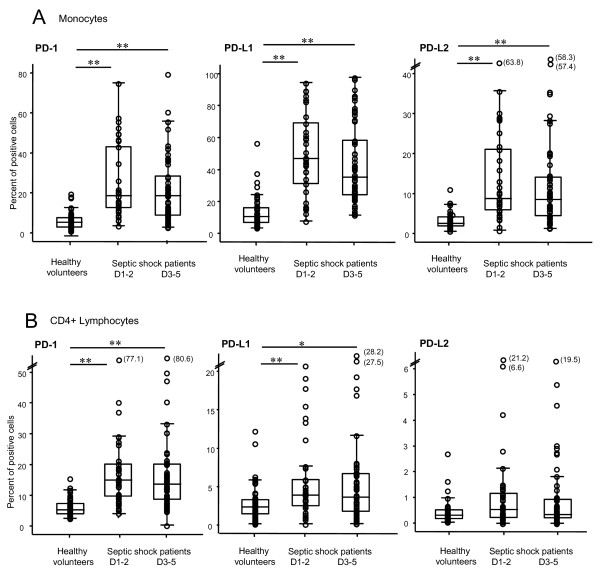
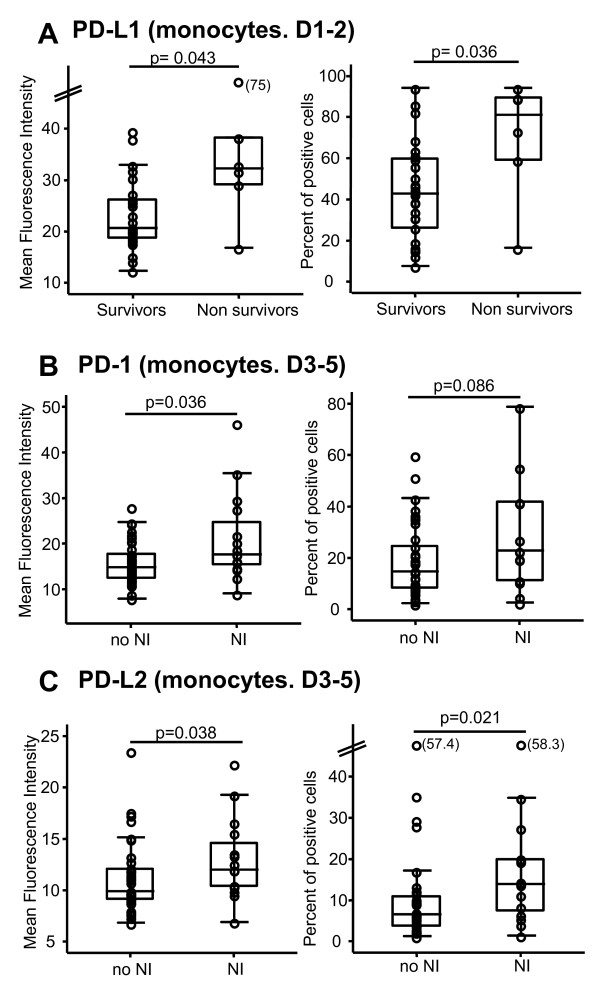
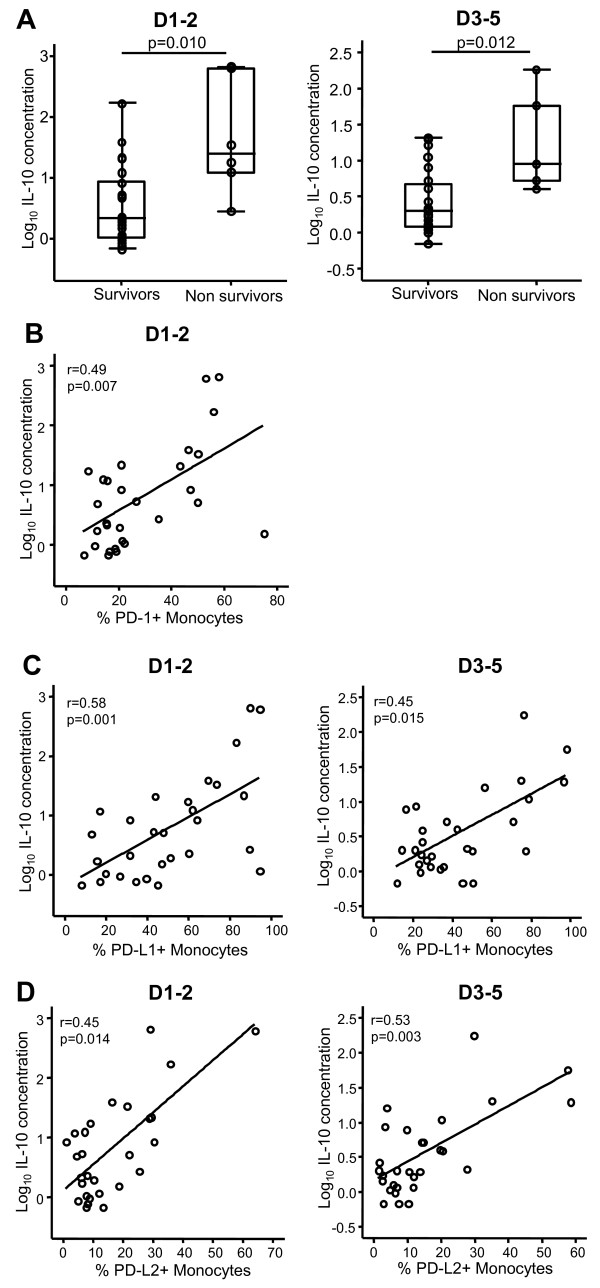
Results: We observed that septic shock patients displayed increased PD-1, PD-Ligand1 (PD-L1) and PD-L2 monocyte expressions and enhanced PD-1 and PD-L1 CD4+ T lymphocyte expressions at day 1-2 and 3-5 after the onset of shock in comparison with patients with trauma and healthy volunteers. Importantly, increased expressions were associated with increased occurrence of secondary nosocomial infections and mortality after septic shock as well as with decreased mitogen-induced lymphocyte proliferation and increased circulating IL-10 concentration.
Conclusions: These findings indicate that PD-1-related molecules may constitute a novel immunoregulatory system involved in sepsis-induced immune alterations. Results should be confirmed in a larger cohort of patients. This may offer innovative therapeutic perspectives on the treatment of this hitherto deadly disease.
Figures
References
-
- Munford RS, Pugin J. Normal responses to injury prevent systemic inflammation and can be immunosuppressive. Am J Respir Crit Care Med. 2001;163:316–321. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
