

Increases in mortality, length of stay, and cost associated with hospital-acquired infections in trauma patients
- PMID: 21422331
- PMCID: PMC3336161
- DOI: 10.1001/archsurg.2011.41
Increases in mortality, length of stay, and cost associated with hospital-acquired infections in trauma patients
Abstract
Objective: To explore the clinical impact and economic burden of hospital-acquired infections (HAIs) in trauma patients using a nationally representative database.
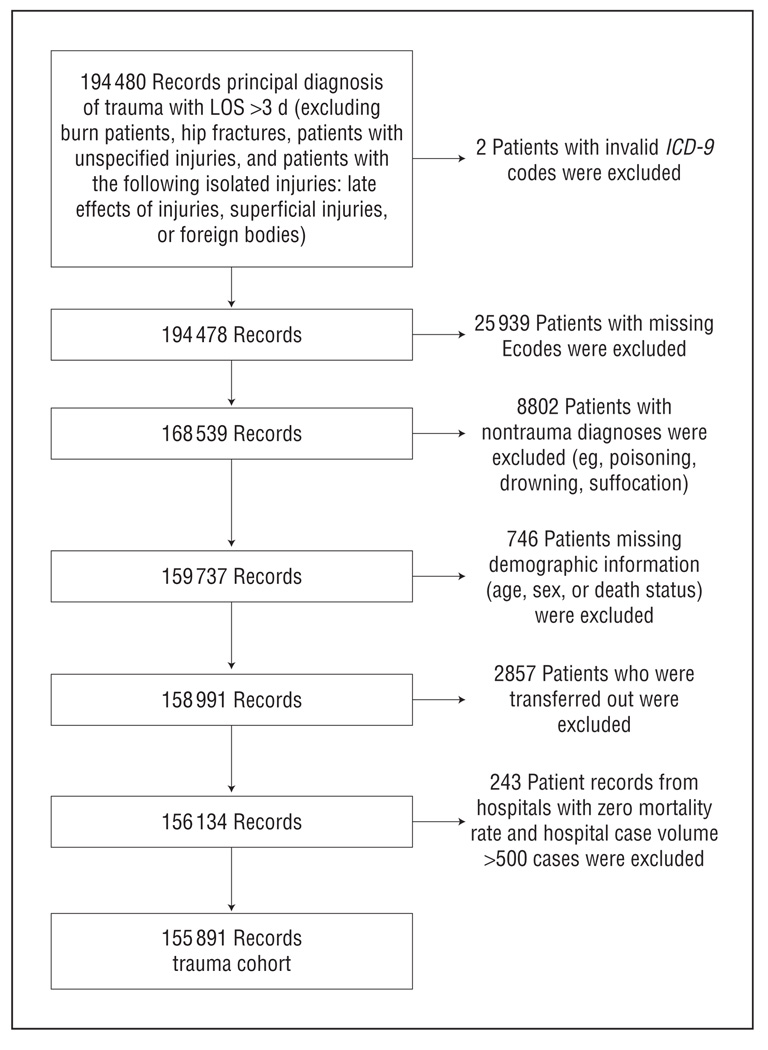
Design: Retrospective study.
Setting: The Healthcare Cost and Utilization Project Nationwide Inpatient Sample.
Patients: Trauma patients.
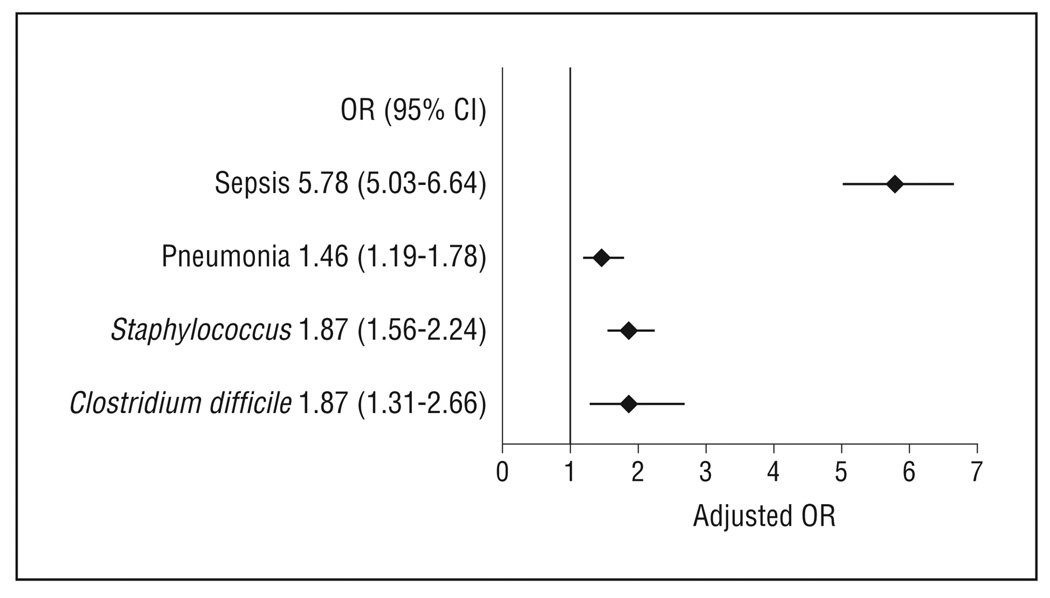
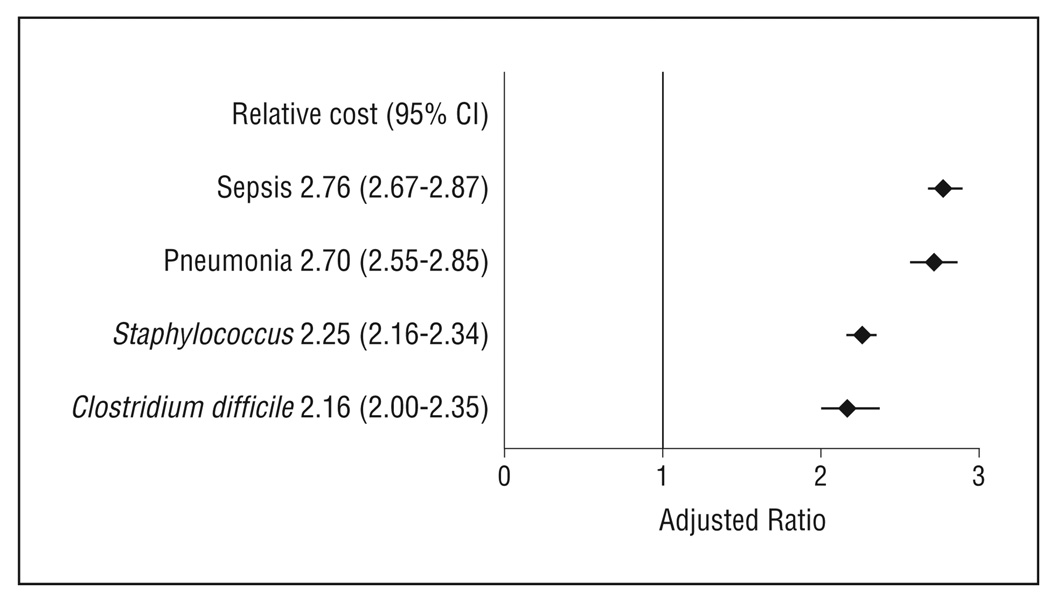
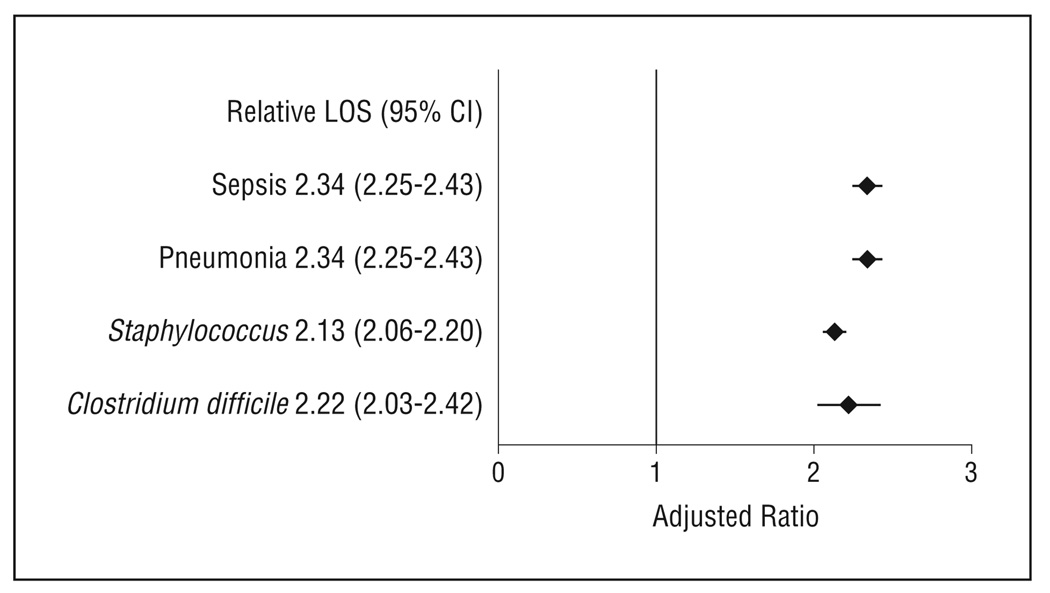
Main outcome measures: We examined the association between HAIs (sepsis, pneumonia, Staphylococcus infections, and Clostridium difficile- associated disease) and in-hospital mortality, length of stay, and inpatient costs using logistic regression and generalized linear models.
Results: After controlling for patient demographics, mechanism of injury, injury type, injury severity, and comorbidities, we found that mortality, cost, and length of stay were significantly higher in patients with HAIs compared with patients without HAIs. Patients with sepsis had a nearly 6-fold higher odds of death compared with patients without an HAI (odds ratio, 5.78; 95% confidence interval, 5.03-6.64; P < .001). Patients with other HAIs had a 1.5- to 1.9-fold higher odds of mortality compared with controls (P < .005). Patients with HAIs had costs that were approximately 2- to 2.5-fold higher compared with patients without HAIs (P < .001). The median length of stay was approximately 2-fold higher in patients with HAIs compared with patients without HAIs (P < .001).
Conclusions: Trauma patients with HAIs are at increased risk for mortality, have longer lengths of stay, and incur higher inpatient costs. In light of the preventability of many HAIs and the magnitude of the clinical and economic burden associated with HAIs, policies aiming to decrease the incidence of HAIs may have a potentially large impact on outcomes in injured patients.
Figures
Comment in
-
Life, liberty, and the pursuit of HAIs.Arch Surg. 2011 Jul;146(7):801. doi: 10.1001/archsurg.2011.42. Arch Surg. 2011. PMID: 21894620 No abstract available.
References
-
- Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
-
- Burke JP. Infection control: a problem for patient safety. N Engl J Med. 2003;348(7):651–656. - PubMed
-
- Scott RD. The direct medical costs of healthcare-associated infections in US hospitals and the benefits of prevention. [Accessed May 5, 2010]; www.cdc.gov/ncidod/dhqp/pdf/Scott_CostPaper.pdf. Published 2009.
-
- Leape LL, Berwick DM. Five years after To Err Is Human: what have we learned? JAMA. 2005;293(19):2384–2390. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
