

Motor subtypes of postoperative delirium in older adults
- PMID: 21422360
- PMCID: PMC3346288
- DOI: 10.1001/archsurg.2011.14
Motor subtypes of postoperative delirium in older adults
Abstract
Hypothesis: Increased knowledge about motor subtypes of delirium may aid clinicians in the management of postoperative geriatric patients.
Design: Prospective cohort study defining preoperative risk factors, outcomes, and adverse events related to motor subtypes of postoperative delirium.
Setting: Referral medical center.
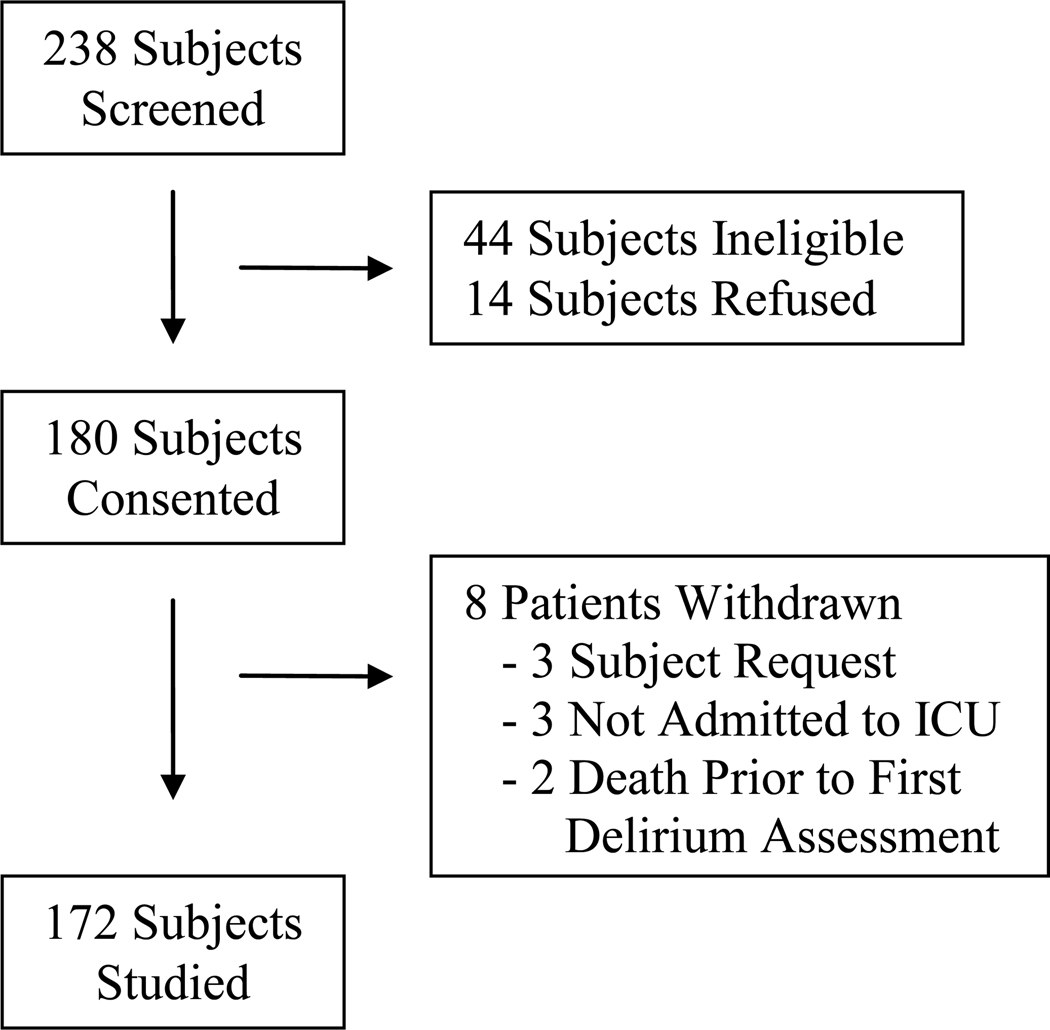
Patients: Persons 50 years and older with planned postoperative intensive care unit (ICU) admission following an elective operation were recruited.
Main outcome measures: Before surgery, a standardized frailty assessment was performed. After surgery, delirium and its motor subtypes were measured using the validated tools of the Confusion Assessment Method-ICU and the Richmond Agitation-Sedation Scale. Statistical analysis included the univariate t and χ(2) tests and analysis of variance with post hoc analysis.
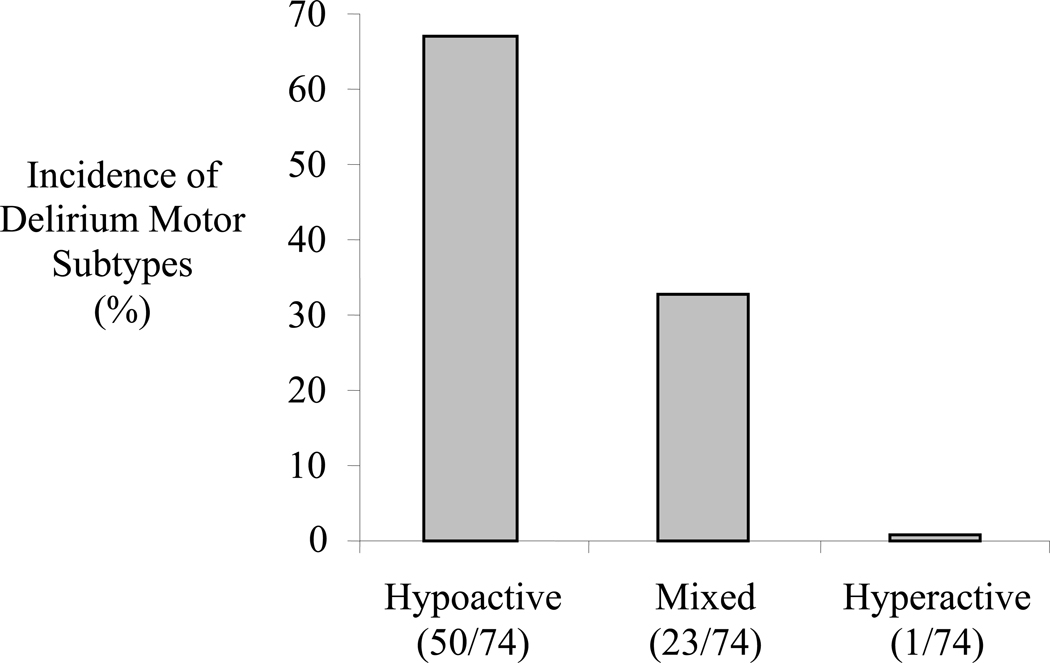
Results: Delirium occurred in 43.0% (74 of 172) of patients, representing 67.6% (50 of 74) hypoactive, 31.1% (23 of 74) mixed, and 1.4% (1 of 74) hyperactive motor subtypes. Compared with those having mixed delirium, patients having hypoactive delirium were older (mean [SD] age, 71 [9] vs 65 [9] years) and more anemic (mean [SD] hematocrit, 36% [8%] vs 41% [6%]) (P = .002 for both). Patients with hypoactive delirium had higher 6-month mortality (32.0% [16 of 50] vs 8.7% [2 of 23], P = .04). Delirium-related adverse events occurred in 24.3% (18 of 74) of patients with delirium; inadvertent tube or line removals occurred more frequently in the mixed group (P = .006), and sacral skin breakdown was more common in the hypoactive group (P = .002).
Conclusions: Motor subtypes of delirium alert clinicians to differing prognosis and adverse event profiles in postoperative geriatric patients. Hypoactive delirium is the most common motor subtype and is associated with worse prognosis (6-month mortality, 1 in 3 patients). Knowledge of differing adverse event profiles can modify clinicians' management of older patients with postoperative delirium.
Figures
Similar articles
-
Motor activity across delirium motor subtypes in geriatric patients assessed using body-worn sensors: a Norwegian cross-sectional study.BMJ Open. 2019 Mar 1;9(2):e026401. doi: 10.1136/bmjopen-2018-026401. BMJ Open. 2019. PMID: 30826800 Free PMC article.
-
Effect of motor subtypes of delirium in the intensive care unit on fast-track failure after cardiac surgery.J Thorac Cardiovasc Surg. 2018 Jan;155(1):268-275.e1. doi: 10.1016/j.jtcvs.2017.08.139. Epub 2017 Sep 30. J Thorac Cardiovasc Surg. 2018. PMID: 29110954
-
Association of Delirium during Critical Illness With Mortality: Multicenter Prospective Cohort Study.Anesth Analg. 2021 Nov 1;133(5):1152-1161. doi: 10.1213/ANE.0000000000005544. Anesth Analg. 2021. PMID: 33929361 Free PMC article.
-
How do predisposing factors differ between delirium motor subtypes? A systematic review and meta-analysis.Age Ageing. 2022 Sep 2;51(9):afac200. doi: 10.1093/ageing/afac200. Age Ageing. 2022. PMID: 36153750 Free PMC article.
-
Distribution of delirium motor subtypes in the intensive care unit: a systematic scoping review.Crit Care. 2022 Mar 3;26(1):53. doi: 10.1186/s13054-022-03931-3. Crit Care. 2022. PMID: 35241132 Free PMC article.
Cited by
-
Delirium Superimposed on Dementia in Perioperative Period and Intensive Care.J Clin Med. 2020 Oct 13;9(10):3279. doi: 10.3390/jcm9103279. J Clin Med. 2020. PMID: 33066174 Free PMC article. Review.
-
Potential Usefulness of Blood Urea Nitrogen to Creatinine Ratio in the Prediction and Early Detection of Delirium Motor Subtype in the Intensive Care Unit.J Clin Med. 2022 Aug 29;11(17):5073. doi: 10.3390/jcm11175073. J Clin Med. 2022. PMID: 36078999 Free PMC article.
-
A call for a more rigorous screening of postoperative delirium.Ann Transl Med. 2019 Sep;7(Suppl 6):S192. doi: 10.21037/atm.2019.07.32. Ann Transl Med. 2019. PMID: 31656771 Free PMC article. No abstract available.
-
Association of Hypoactive and Hyperactive Delirium With Cognitive Function After Critical Illness.Crit Care Med. 2020 Jun;48(6):e480-e488. doi: 10.1097/CCM.0000000000004313. Crit Care Med. 2020. PMID: 32317589 Free PMC article.
-
Management of proximal femur fractures in the elderly: current concepts and treatment options.Eur J Med Res. 2021 Aug 4;26(1):86. doi: 10.1186/s40001-021-00556-0. Eur J Med Res. 2021. PMID: 34348796 Free PMC article. Review.
References
-
- Marcantonio ER, Juarez G, Goldman L, et al. The relationship of postoperative delirium with psychoactive medications. JAMA. 1994;272(19):1518–1522. - PubMed
-
- Geriatric Review Syllabus - A Core Curriculum in Geriatric Medicine. Sixth Edition ed. New York: American Geriatrics Society; 2006.
-
- Robinson TN, Raeburn CD, Tran ZV, et al. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg. 2009;249(1):173–178. - PubMed
-
- Dasgupta M, Dumbrell AC. Preoperative risk assessment for delirium after noncardiac surgery: a systematic review. J Am Geriatr Soc. 2006;54(10):1578–1589. - PubMed
-
- Lipowski ZJ. Transient cognitive disorders (delirium, acute confusional states) in the elderly. Am J Psychiatry. 1983;140(11):1426–1436. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
