

Cardiorespiratory fitness and classification of risk of cardiovascular disease mortality
- PMID: 21422392
- PMCID: PMC3926656
- DOI: 10.1161/CIRCULATIONAHA.110.003236
Cardiorespiratory fitness and classification of risk of cardiovascular disease mortality
Abstract
Background: Cardiorespiratory fitness (fitness) is associated with cardiovascular disease (CVD) mortality. However, the extent to which fitness improves risk classification when added to traditional risk factors is unclear.
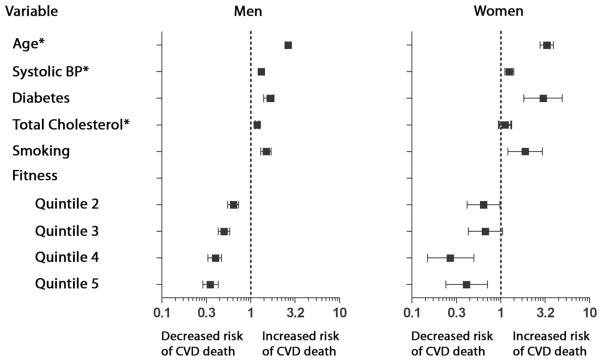
Methods and results: Fitness was measured by the Balke protocol in 66 371 subjects without prior CVD enrolled in the Cooper Center Longitudinal Study between 1970 and 2006; follow-up was extended through 2006. Cox proportional hazards models were used to estimate the risk of CVD mortality with a traditional risk factor model (age, sex, systolic blood pressure, diabetes mellitus, total cholesterol, and smoking) with and without the addition of fitness. The net reclassification improvement and integrated discrimination improvement were calculated at 10 and 25 years. Ten-year risk estimates for CVD mortality were categorized as <1%, 1% to <5%, and ≥5%, and 25-year risk estimates were categorized as <8%, 8% to 30%, and ≥30%. During a median follow-up period of 16 years, there were 1621 CVD deaths. The addition of fitness to the traditional risk factor model resulted in reclassification of 10.7% of the men, with significant net reclassification improvement at both 10 years (net reclassification improvement=0.121) and 25 years (net reclassification improvement=0.041) (P<0.001 for both). The integrated discrimination improvement was 0.010 at 10 years (P<0.001), and the relative integrated discrimination improvement was 29%. Similar findings were observed for women at 25 years.
Conclusions: A single measurement of fitness significantly improves classification of both short-term (10-year) and long-term (25-year) risk for CVD mortality when added to traditional risk factors.
Conflict of interest statement
Dr Berry reports receiving speaker’s fees from Merck/Schering-Plough. The other authors have no conflict of interest to disclose.
Figures
Comment in
-
How will exercise capacity gain enough respect?Circulation. 2011 Apr 5;123(13):1364-6. doi: 10.1161/CIRCULATIONAHA.111.023218. Epub 2011 Mar 21. Circulation. 2011. PMID: 21422388 No abstract available.
References
-
- Physical Activity Guidelines for Americans. U.S. Department of Health and Human Services; 2008. [Accessed January 10, 2011]. http://www.health.gov/paguidelines. Last updated August 21, 2009.
-
- Dorn J, Naughton J, Imamura D, Trevisan M. Results of a multicenter randomized clinical trial of exercise and long-term survival in myocardial infarction patients: the National Exercise and Heart Disease Project (NEHDP) Circulation. 1999;100:1764–1769. - PubMed
-
- Erikssen G, Liestol K, Bjornholt J, Thaulow E, Sandvik L, Erikssen J. Changes in physical fitness and changes in mortality. Lancet. 1998;352:759–762. - PubMed
-
- Paffenbarger RS, Jr, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med. 1993;328:538–545. - PubMed
-
- Aktas MK, Ozduran V, Pothier CE, Lang R, Lauer MS. Global risk scores and exercise testing for predicting all-cause mortality in a preventive medicine program. JAMA. 2004;292:1462–1468. - PubMed
