

Effectiveness of the standard WHO recommended retreatment regimen (category II) for tuberculosis in Kampala, Uganda: a prospective cohort study
- PMID: 21423586
- PMCID: PMC3058098
- DOI: 10.1371/journal.pmed.1000427
Effectiveness of the standard WHO recommended retreatment regimen (category II) for tuberculosis in Kampala, Uganda: a prospective cohort study
Abstract
Background: Each year, 10%-20% of patients with tuberculosis (TB) in low- and middle-income countries present with previously treated TB and are empirically started on a World Health Organization (WHO)-recommended standardized retreatment regimen. The effectiveness of this retreatment regimen has not been systematically evaluated.
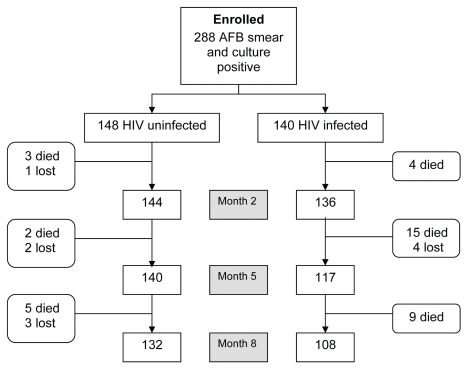
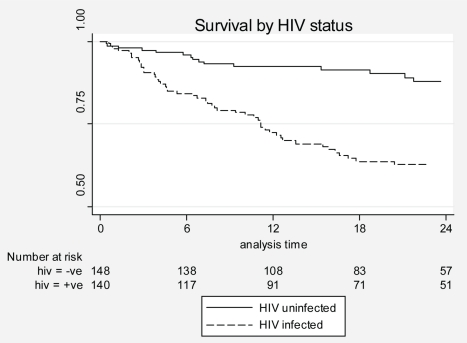
Methods and findings: From July 2003 to January 2007, we enrolled smear-positive, pulmonary TB patients into a prospective cohort to study treatment outcomes and mortality during and after treatment with the standardized retreatment regimen. Median time of follow-up was 21 months (interquartile range 12-33 months). A total of 29/148 (20%) HIV-uninfected and 37/140 (26%) HIV-infected patients had an unsuccessful treatment outcome. In a multiple logistic regression analysis to adjust for confounding, factors associated with an unsuccessful treatment outcome were poor adherence (adjusted odds ratio [aOR] associated with missing half or more of scheduled doses 2.39; 95% confidence interval (CI) 1.10-5.22), HIV infection (2.16; 1.01-4.61), age (aOR for 10-year increase 1.59; 1.13-2.25), and duration of TB symptoms (aOR for 1-month increase 1.12; 1.04-1.20). All patients with multidrug-resistant TB had an unsuccessful treatment outcome. HIV-infected individuals were more likely to die than HIV-uninfected individuals (p<0.0001). Multidrug-resistant TB at enrollment was the only common risk factor for death during follow-up for both HIV-infected (adjusted hazard ratio [aHR] 17.9; 6.0-53.4) and HIV-uninfected (14.7; 4.1-52.2) individuals. Other risk factors for death during follow-up among HIV-infected patients were CD4<50 cells/ml and no antiretroviral treatment (aHR 7.4, compared to patients with CD4≥200; 3.0-18.8) and Karnofsky score <70 (2.1; 1.1-4.1); and among HIV-uninfected patients were poor adherence (missing half or more of doses) (3.5; 1.1-10.6) and duration of TB symptoms (aHR for a 1-month increase 1.9; 1.0-3.5).
Conclusions: The recommended regimen for retreatment TB in Uganda yields an unacceptable proportion of unsuccessful outcomes. There is a need to evaluate new treatment strategies in these patients.
© 2011 Jones-Lo´pez et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
The challenge of discharging research ethics duties in resource-constrained settings.PLoS Med. 2011 Mar;8(3):e1000421. doi: 10.1371/journal.pmed.1000421. Epub 2011 Mar 15. PLoS Med. 2011. PMID: 21423584 Free PMC article.
References
-
- Mak A, Thomas A, Del Granado M, Zaleskis R, Mouzafarova N, et al. Influence of multidrug resistance on tuberculosis treatment outcomes with standardized regimens. Am J Respir Crit Care Med. 2008;178:306–312. - PubMed
-
- World Health Organization. Global tuberculosis control - a short update to the 2009 report. Geneva: World Health Organization; 2009.
-
- Menzies D, Benedetti A, Paydar A, Royce S, Pai M, et al. Standardized treatment of active tuberculosis in patients with previous treatment and/or with mono-resistance to isoniazid: a systematic review and meta-analysis. PLoS Med. 2009;6:e1000150. doi: 10.1371/journal.pmed.1000150. - DOI - PMC - PubMed
-
- Rouillon A. The Mutual Assistance Programme of the IUATLD. Development, contribution and significance. Bull Int Union Tuberc Lung Dis. 1991;66:159–172. - PubMed
-
- World Health Organization. Treatment of tuberculosis: guidelines – 4th edition. Geneva: World Health Organization; 2009.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
