

Antitumor activity of Noscapine in combination with Doxorubicin in triple negative breast cancer
- PMID: 21423660
- PMCID: PMC3057970
- DOI: 10.1371/journal.pone.0017733
Antitumor activity of Noscapine in combination with Doxorubicin in triple negative breast cancer
Abstract
Background: The aim of this study was to investigate the anticancer activity and mechanism of action of Noscapine alone and in combination with Doxorubicin against triple negative breast cancer (TNBC).
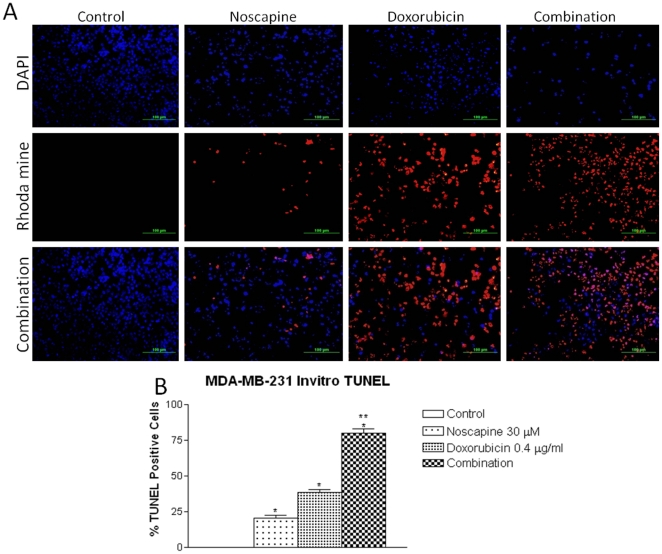
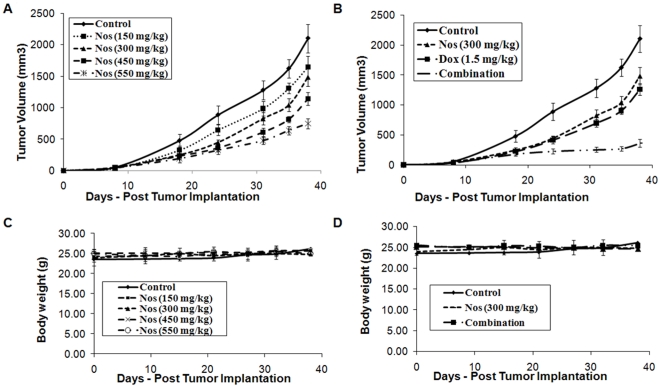
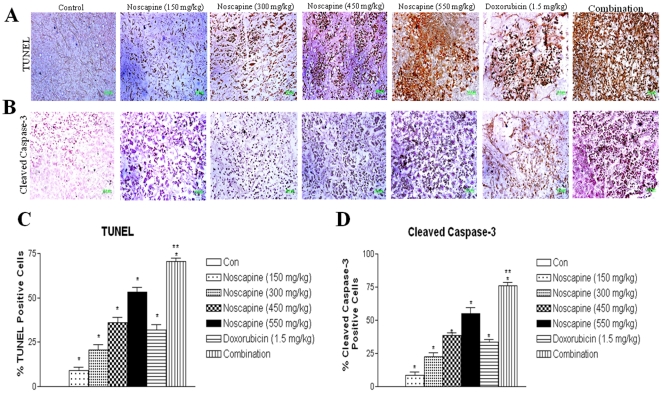
Methods: TNBC cells were pretreated with Noscapine or Doxorubicin or combination and combination index values were calculated using isobolographic method. Apoptosis was assessed by TUNEL staining. Female athymic Nu/nu mice were xenografted with MDA-MB-231 cells and the efficacy of Noscapine, Doxorubicin and combination was determined. Protein expression, immunohistochemical staining were evaluated in harvested tumor tissues.
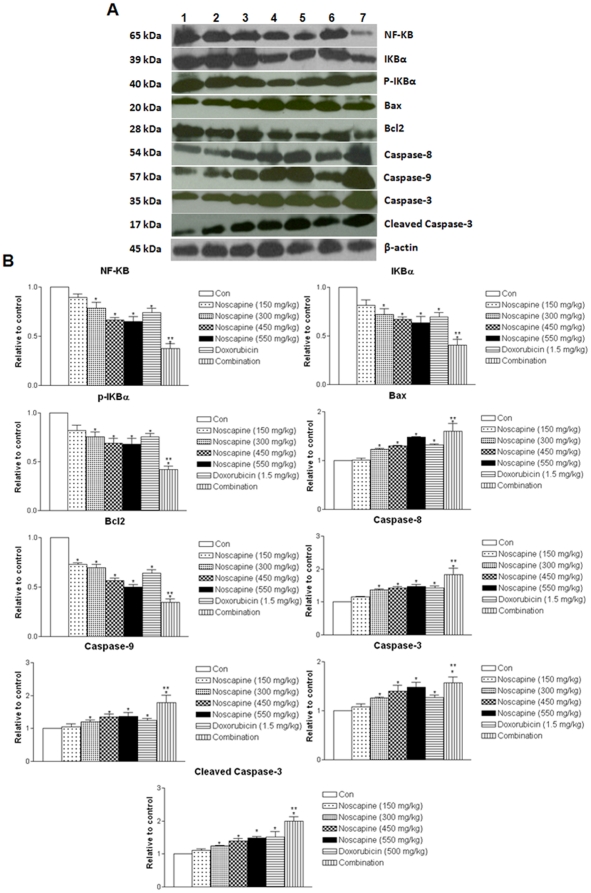
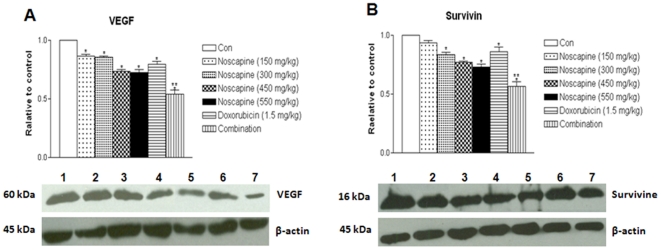
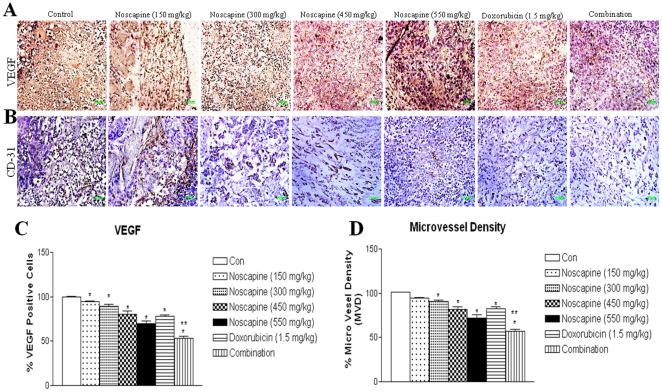
Results: Noscapine inhibited growth of MDA-MB-231 and MDA-MB-468 cells with the IC(50) values of 36.16±3.76 and 42.7±4.3 µM respectively. The CI values (<0.59) were suggestive of strong synergistic interaction between Noscapine and Doxorubicin and combination treatment showed significant increase in apoptotic cells. Noscapine showed dose dependent reduction in the tumor volumes at a dose of 150-550 mg/kg/day compared to controls. Noscapine (300 mg/kg), Doxorubicin (1.5 mg/kg) and combination treatment reduced tumor volume by 39.4±5.8, 34.2±5.7 and 82.9±4.5 percent respectively and showed decreased expression of NF-KB pathway proteins, VEGF, cell survival, and increased expression of apoptotic and growth inhibitory proteins compared to single-agent treatment and control groups.
Conclusions: Noscapine potentiated the anticancer activity of Doxorubicin in a synergistic manner against TNBC tumors via inactivation of NF-KB and anti-angiogenic pathways while stimulating apoptosis. These findings suggest potential benefit for use of oral Noscapine and Doxorubicin combination therapy for treatment of more aggressive TNBC.
Conflict of interest statement
Figures
References
-
- Kassam F, Enright K, Dent R, Dranitsaris G, Myers J, et al. Survival outcomes for patients with metastatic triple-negative breast cancer: implications for clinical practice and trial design. Clin Breast Cancer. 2009;9:29–33. - PubMed
-
- Irvin WJ, Jr, Carey LA. What is triple-negative breast cancer? Eur J Cancer. 2008;44:2799–2805. - PubMed
-
- Stockmans G, Deraedt K, Wildiers H, Moerman P, Paridaens R. Triple-negative breast cancer. Curr Opin Oncol. 2008;20:614–620. - PubMed
-
- Moulder S, Hortobagyi GN. Advances in the treatment of breast cancer. Clin Pharmacol Ther. 2008;83:26–36. - PubMed
-
- Buzdar AU. Advances in endocrine treatments for postmenopausal women with metastatic and early breast cancer. Oncologist. 2003;8:335–341. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
