

doi: 10.4103/0971-3026.73543.
Malignant brachial plexopathy: A pictorial essay of MRI findings
Affiliations
- PMID: 21423902
- PMCID: PMC3056624
- DOI: 10.4103/0971-3026.73543
Item in Clipboard
Malignant brachial plexopathy: A pictorial essay of MRI findings
Indian J Radiol Imaging.
2010 Nov.
Abstract
For imaging, the brachial plexus is a technically and anatomically challenging region of the peripheral nervous system. MRI has a central role in the identification and accurate characterization of malignant lesions arising here, as also in defining their extent and the status of the adjacent structures. The purpose of this pictorial essay is to describe the MRI features of primary and secondary malignant brachial plexopathies and radiation-induced brachial nerve damage.
Keywords: Brachial plexus; MRI; malignant peripheral nerve sheath tumor; radiation-induced plexopathy.
Conflict of interest statement
Figures
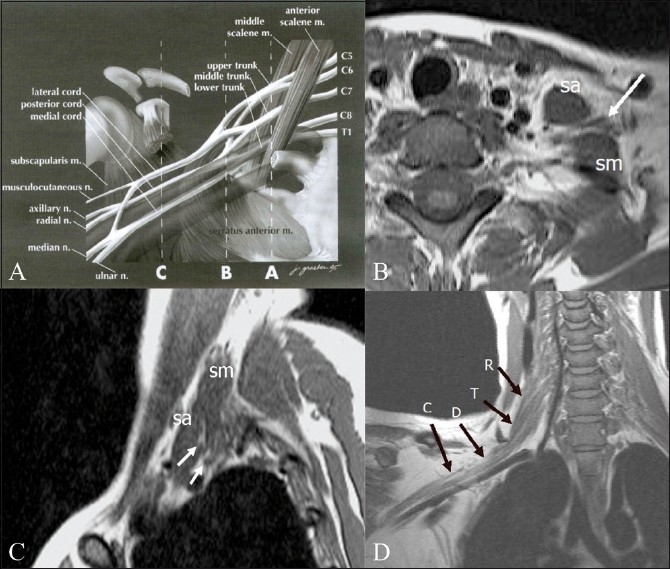
Diagrammatic representation (A) of the anatomy of the brachial plexus, with the musculoskeletal and vascular landmarks indicated by three interrupted lines: A — sagittal plane that intersects the interscalene triangle, B — sagittal plane through the lateral margin of the first rib, and C — sagittal plane of the coracoid process. (m, muscle; n, nerve). Axial (B) and sagittal (C), T1W images of the plexus in the interscalene triangle. The anterior and middle scalene muscles are the boundaries of the interscalene triangle and act as useful radiological landmarks for locating the roots and trunks (arrows) of the brachial plexus that lie within the triangle. (sa: scalenus anterior; sm: scalenus medius.) Oblique coronal T1W image (D) shows the roots (R), trunks (T), divisions (D), and cords (C) of the right brachial plexus. A — Reprinted from Neuroimaging Clinics of North America, 14(1), Bowen BC, Pattany PM, Saraf-Lavi E, and Maravilla KR, The brachial plexus: normal anatomy, pathology, and MR imaging, page 27, Copyright 2004. With permission from Elsevier
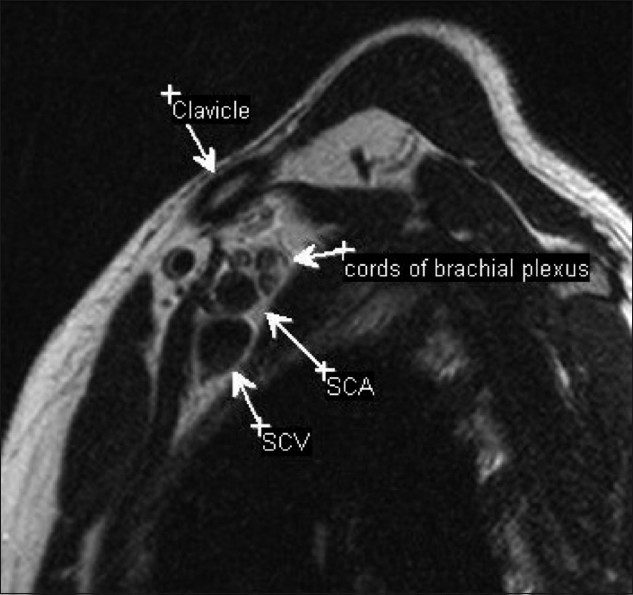
Sagittal T2W image through the axilla showing the relationship of the cords to the vessels. In the axilla, the three cords are identified posterosuperior to the vessels. (SCA: subclavian artery; SCV: subclavian vein)
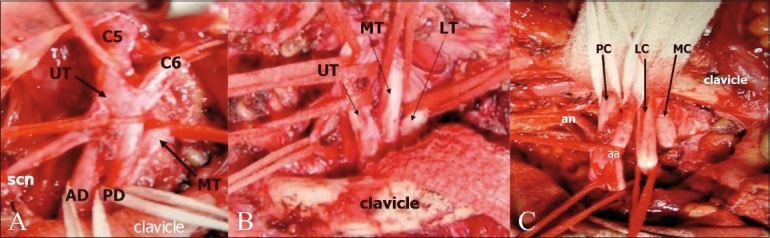
The surgical anatomy is based on the relationship of the brachial plexus to the clavicle. Intraoperative photographs show the supraclavicular (A), retroclavicular (B), and infraclavicular (C) portions of the brachial plexus. (Photograph courtesy: Ketan Desai, Department of Neurosurgery, Seth GS Medical College and KEM Hospital) (UT: upper trunk; MT: middle trunk; LT: lower trunk; AD: anterior division; PD: posterior division; scn: suprascapular nerve; PC: posterior cord; LC: lateral cord; MC: medial cord; an: axillary nerve, and aa: axillary artery)
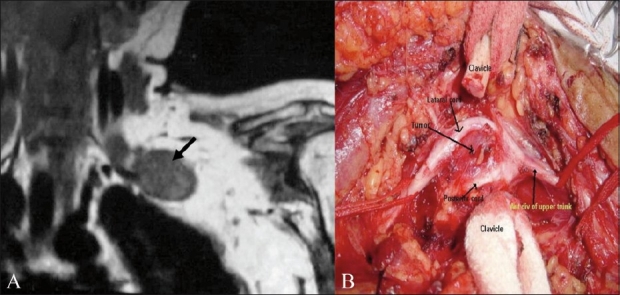
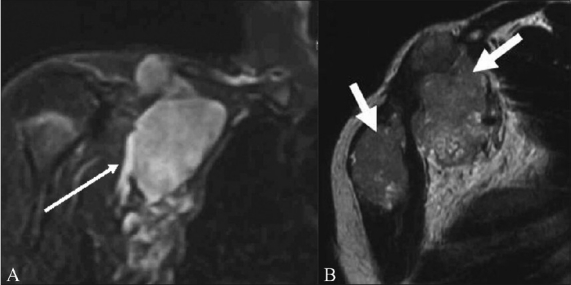
A 57-year-old male with histopathologically proven malignant schwannoma. Preoperative coronal T1W MRI (A) shows a well-marginated. low-signal-intensity solid mass (arrow) arising from the plexus. The corresponding intraoperative photograph (B) shows the tumor (arrow) seen after dividing the clavicle. The mass splays the lateral and posterior cords. (Photograph courtesy: Ketan Desai, Department of Neurosurgery, Seth GS Medical College and KEM Hospital)
A 59-year-old male with neurofibrosarcoma involving the right brachial plexus. Coronal STIR (A) image shows a large heterogeneous, predominantly hyperintense, mass arising from the right brachial plexus (arrows). Focal linear low-signal septae are seen within. Contrast-enhanced, fat-suppressed, axial (B) image shows the mass enhancing intensely; it is dumbell-shaped, with a small intraspinal component that indents the thecal sac, and a large paravertebral component
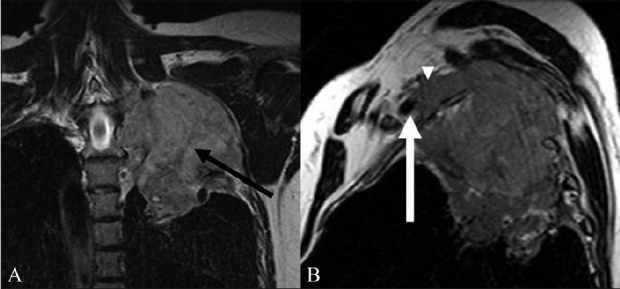
A 60-year-old male with Pancoast tumor. Coronal T2W (A) image shows a tumor of the apex of the left lung extending into the supraclavicular fossa to involve the trunks and divisions of the left brachial plexus (arrow). The mass is solid, with an intermediate T2 signal. The Sagittal T2W (B) image shows the anterosuperior component of the mass involving the divisions of the brachial plexus (arrowhead) posterosuperior to the subclavian vessels. The mass abuts the left subclavian artery (arrow)
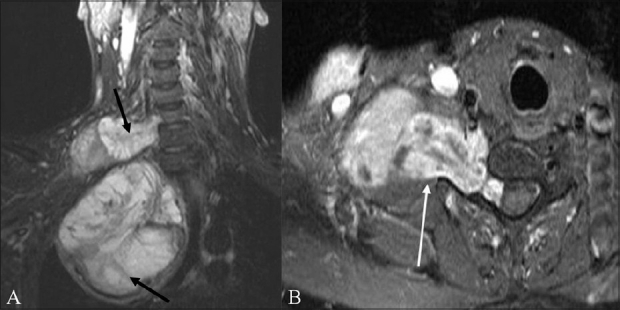
A 62-year-old male with a soft tissue sarcoma of the chest wall and axilla. The coronal STIR (A) and axial T2W (B) images show a hyperintense mass that infiltrates the cords of the brachial plexus with encasement of the axillary vessels (arrow)

A 43-year-old female with metastatic breast cancer. Axial fat-suppressed, contrast-enhanced T1W (A) image shows abnormal enhancing soft tissue metastases along the right anterior chest wall, partially encasing the trunks of the right brachial plexus (arrowheads). Also seen in this image are bilateral enhancing pulmonary metastases (arrows). The abnormal perineural soft tissue (arrow) extends into the axilla, encasing the divisions and cords of the plexus, as seen on the sagittal fat-suppressed T1W image (B)
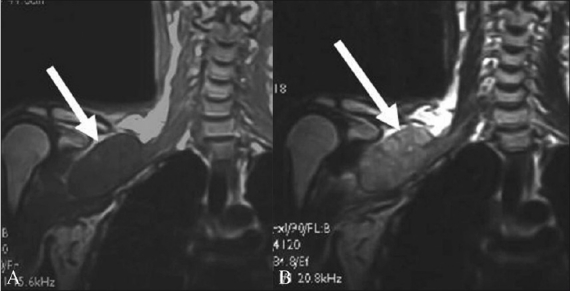
A 71-year-old male with buccal squamous cell carcinoma and supraclavicular lymph node metastasis. The coronal T1W (A) image shows a low-signal-intensity metastatic lymph nodal mass compressing the trunks, divisions, and cords of the right brachial plexus (arrow). On the corresponding coronal T2W (B) image, the mass shows high intensity (arrow)
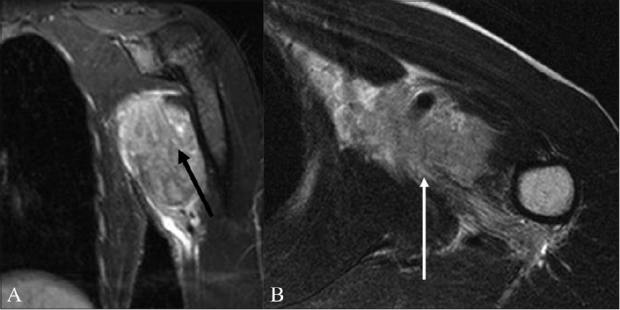
A 50-year-old-male with lymphoma. Coronal STIR (A) image shows a large multilobulated nodal mass involving the right brachial plexus (arrow). Sagittal T2W (B) image shows the lymph nodal mass encasing the divisions of the brachial plexus and the adjacent subclavian artery and vein (arrow)
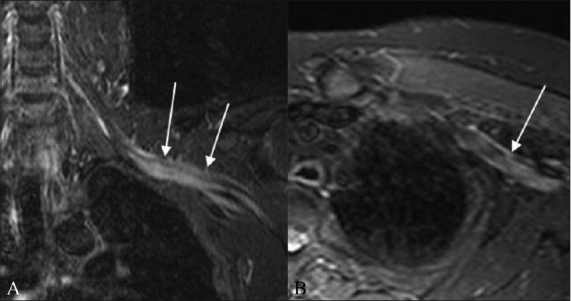
A 52-year-old-male with biopsy-proven neurolymphomatosis. Coronal (A) and axial (B) STIR images show thickening and increased signal in the left brachial plexus (arrows)
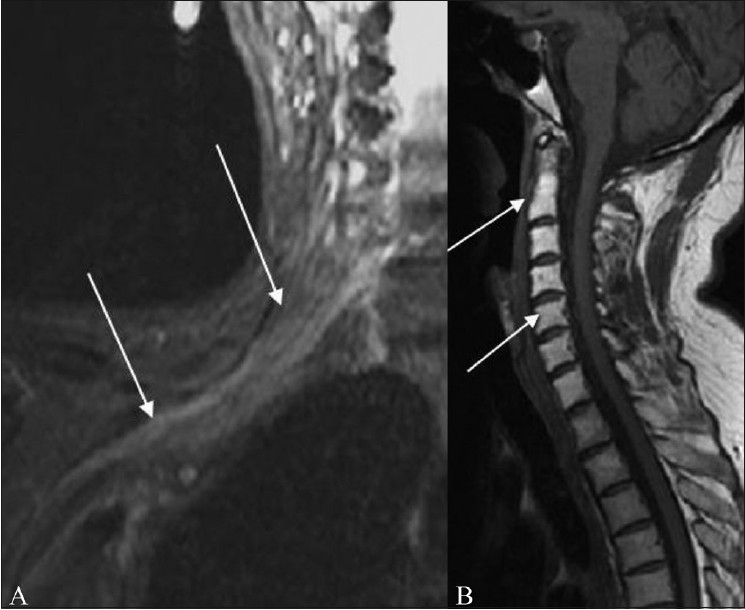
A 60-year-old female presenting with right upper limb weakness 18 months after radiation therapy for breast cancer. Coronal fat-suppressed T2W image (A) shows radiation plexopathy appearing as an abnormal thickening, and increased signal in the right brachial plexus (arrow). Sagittal T1W image (B) shows radiation-induced fat marrow replacement in the cervical vertebrae (arrows)
References
-
- Todd M, Shah GV, Mukherji SK. MR imaging of brachial plexus. Top Magn Reson Imaging. 2004;15:113–25. - PubMed
-
- Wittenberg KH, Adkins MC. MR imaging of nontraumatic brachial plexopathies: frequency and spectrum of findings. Radiographics. 2000;20:1023–32. - PubMed
-
- Shearer P, Parham D, Kovnar E, Kun L, Rao B, Lobe T, et al. Neurofibromatosis type I and malignancy: review of 32 pediatric cases treated at a single institution. Med Pediatr Oncol. 1994;22:78–83. - PubMed
-
- Hayes CE, Tsuruda JS, Mathis CM, Maravilla KR, Kliot M, Filler AG. Brachial plexus: MR imaging with a dedicated phased array of surface coils. Radiology. 1997;203:286–9. - PubMed
-
- Castillo M. Imaging the anatomy of the brachial plexus: review and self-assessment module. AJR Am J Roentgenol. 2005;185:S196–204. - PubMed
LinkOut - more resources
Full Text Sources