

Histological heterogeneity of glomerular segmental lesions in focal segmental glomerulosclerosis
- PMID: 21424374
- PMCID: PMC3253997
- DOI: 10.1007/s11255-011-9932-y
Histological heterogeneity of glomerular segmental lesions in focal segmental glomerulosclerosis
Abstract
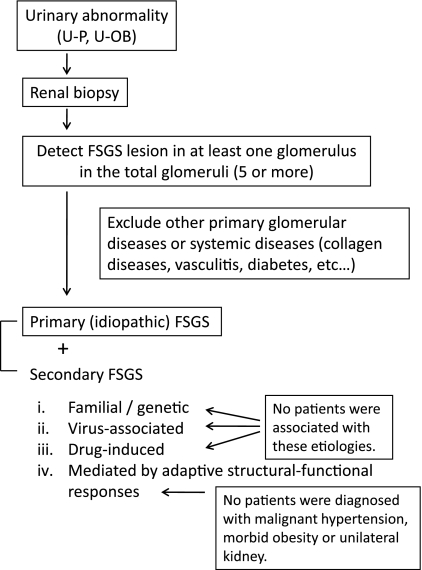
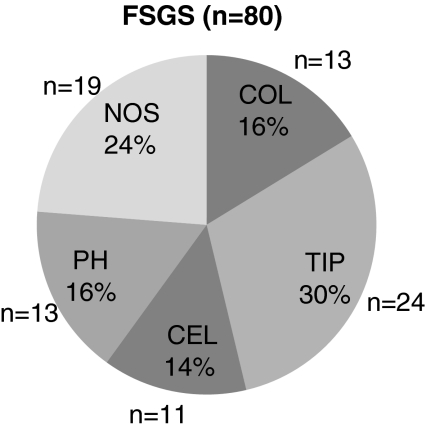
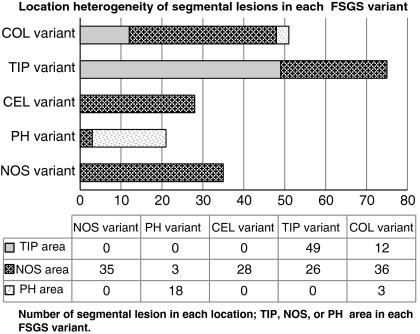
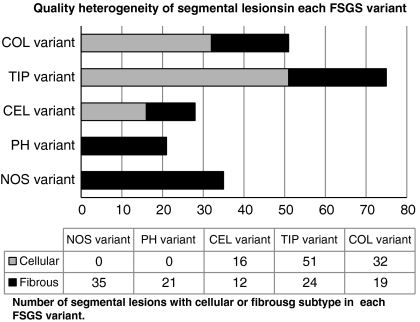
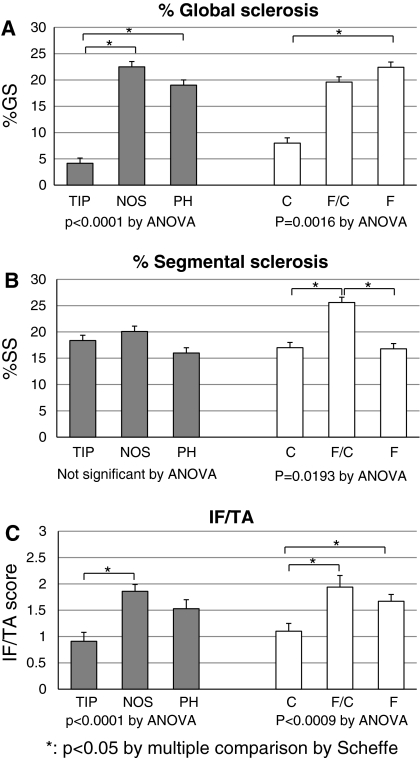
Focal segmental glomerulosclerosis (FSGS) involves considerable histological heterogeneity in terms of location and quality of the glomerular segmental lesions. The present study investigated the heterogeneity of segmental lesions in each variant of FSGS, determined by the Columbia classification, and its clinical relevance. All glomerular segmental lesions of 80 cases of primary FSGS were evaluated histologically based on location [tip (TIP), perihilar (PH), or not otherwise specified (NOS)], and quality (cellular or fibrous). Among the 1,299 glomeruli of the 80 biopsy specimens, 210 glomeruli (16.2%) had segmental lesions, comprising 57 (27%) cellular TIP, 4 (2%) fibrous TIP, 42 (20%) cellular NOS, 86 (41%) fibrous NOS, and 21 (10%) fibrous PH lesions. Each case was also classified into one of the five histological variants of the Columbia classification: collapsing (COL), TIP, cellular (CEL), PH, or NOS. Overlap of segmental lesions in different location categories was seen in the COL, TIP, and PH variants, and heterogeneity of quality was apparent in the COL and CEL variants. Histological findings of the CEL variant (endocapillary hypercellularity) were observed in nine of the 13 COL variants. Both location and quality correlated with disease duration, degree of proteinuria, and histological severity of global glomerular sclerosis and tubulo-interstitial lesions. These results demonstrated the histological heterogeneity of glomerular segmental lesions in all variants of the Columbia classification, except NOS. However, the fidelity of location and dominance of histological features were generally conserved in the TIP and PH variants. The COL and CEL variants warrant further investigation because of their overlapping histological findings and apparent histological heterogeneity in the glomerular segmental lesions.
Figures




References
-
- Schwartz MM, Evans J, Bain R, et al. Focal segmental glomerulosclerosis: prognostic implications of the cellular lesion. J Am Soc Nephrol. 1999;10:1900–1907. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
