

Sequential therapy with JX-594, a targeted oncolytic poxvirus, followed by sorafenib in hepatocellular carcinoma: preclinical and clinical demonstration of combination efficacy
- PMID: 21427706
- PMCID: PMC3129795
- DOI: 10.1038/mt.2011.39
Sequential therapy with JX-594, a targeted oncolytic poxvirus, followed by sorafenib in hepatocellular carcinoma: preclinical and clinical demonstration of combination efficacy
Abstract
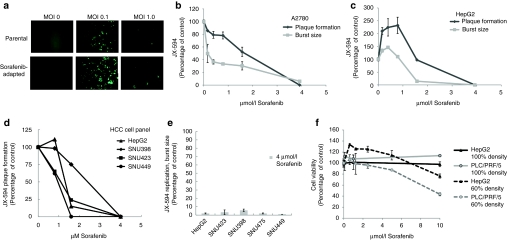
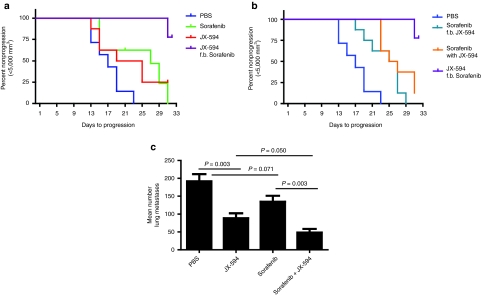
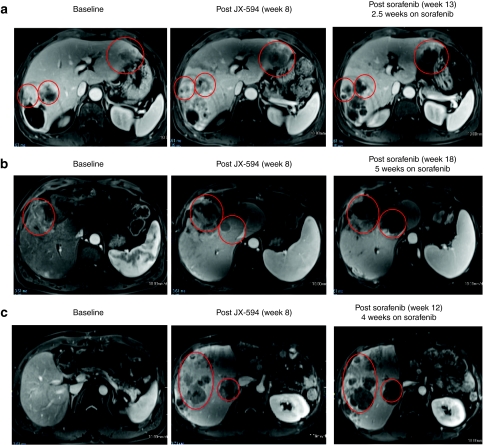
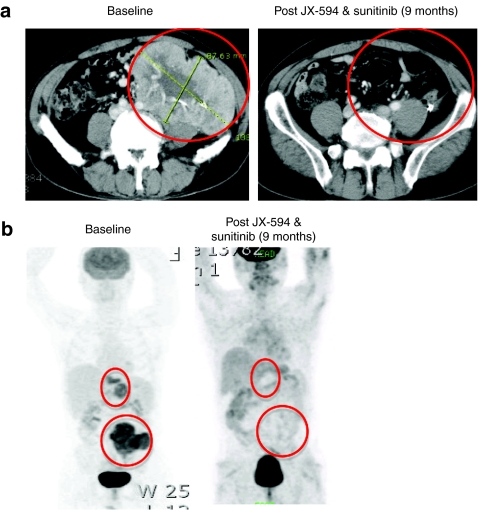
JX-594 is a targeted and granulocyte-macrophage colony stimulating factor (GM-CSF) expressing oncolytic poxvirus designed to selectively replicate in and destroy cancer cells through viral oncolysis and tumor-specific immunity. In a phase 1 trial, JX-594 injection into hepatocellular carcinoma (HCC) was well-tolerated and associated with viral replication, decreased tumor perfusion, and tumor necrosis. We hypothesized that JX-594 and sorafenib, a small molecule inhibitor of B-raf and vascular endothelial growth factor receptor (VEGFR) approved for HCC, would have clinical benefit in combination given their demonstrated efficacy in HCC patients and their complementary mechanisms-of-action. HCC cell lines were uniformly sensitive to JX-594. Anti-raf kinase effects of concurrent sorafenib inhibited JX-594 replication in vitro, whereas sequential therapy was superior to either agent alone in murine tumor models. We therefore explored pilot safety and efficacy of JX-594 followed by sorafenib in three HCC patients. In all three patients, sequential treatment was (i) well-tolerated, (ii) associated with significantly decreased tumor perfusion, and (iii) associated with objective tumor responses (Choi criteria; up to 100% necrosis). HCC historical control patients on sorafenib alone at the same institutions had no objective tumor responses (0 of 15). Treatment of HCC with JX-594 followed by sorafenib has antitumoral activity, and JX-594 may sensitize tumors to subsequent therapy with VEGF/VEGFR inhibitors.
Figures

Similar articles
-
Oncolytic immunotherapy using recombinant vaccinia virus GLV-1h68 kills sorafenib-resistant hepatocellular carcinoma efficiently.Surgery. 2014 Aug;156(2):263-9. doi: 10.1016/j.surg.2014.03.031. Epub 2014 Jun 21. Surgery. 2014. PMID: 24957667 Free PMC article.
-
The targeted oncolytic poxvirus JX-594 demonstrates antitumoral, antivascular, and anti-HBV activities in patients with hepatocellular carcinoma.Mol Ther. 2008 Sep;16(9):1637-42. doi: 10.1038/mt.2008.143. Epub 2008 Jul 15. Mol Ther. 2008. PMID: 18628758
-
Use of a targeted oncolytic poxvirus, JX-594, in patients with refractory primary or metastatic liver cancer: a phase I trial.Lancet Oncol. 2008 Jun;9(6):533-42. doi: 10.1016/S1470-2045(08)70107-4. Epub 2008 May 19. Lancet Oncol. 2008. PMID: 18495536 Clinical Trial.
-
Selection of patients with hepatocellular carcinoma for sorafenib.J Natl Compr Canc Netw. 2009 Apr;7(4):397-403. doi: 10.6004/jnccn.2009.0028. J Natl Compr Canc Netw. 2009. PMID: 19406040 Review.
-
Preclinical and clinical development of the oral multikinase inhibitor sorafenib in cancer treatment.Drugs Today (Barc). 2005 Dec;41(12):773-84. doi: 10.1358/dot.2005.41.12.937959. Drugs Today (Barc). 2005. PMID: 16474853 Review.
Cited by
-
The Thr300Ala variant in ATG16L1 is associated with improved survival in human colorectal cancer and enhanced production of type I interferon.Gut. 2016 Mar;65(3):456-64. doi: 10.1136/gutjnl-2014-308735. Epub 2015 Feb 2. Gut. 2016. PMID: 25645662 Free PMC article.
-
Overcoming Tumor Resistance to Oncolyticvaccinia Virus with Anti-PD-1-Based Combination Therapy by Inducing Antitumor Immunity in the Tumor Microenvironment.Vaccines (Basel). 2020 Jun 19;8(2):321. doi: 10.3390/vaccines8020321. Vaccines (Basel). 2020. PMID: 32575351 Free PMC article.
-
Oncolytic virus therapy in cancer: A current review.World J Virol. 2021 Sep 25;10(5):229-255. doi: 10.5501/wjv.v10.i5.229. World J Virol. 2021. PMID: 34631474 Free PMC article. Review.
-
T-cell engager-armed oncolytic vaccinia virus significantly enhances antitumor therapy.Mol Ther. 2014 Jan;22(1):102-11. doi: 10.1038/mt.2013.240. Epub 2013 Oct 17. Mol Ther. 2014. PMID: 24135899 Free PMC article.
-
Evolutionary cancer-favoring engineered vaccinia virus for metastatic hepatocellular carcinoma.Oncotarget. 2017 Apr 20;8(42):71489-71499. doi: 10.18632/oncotarget.17288. eCollection 2017 Sep 22. Oncotarget. 2017. PMID: 29069721 Free PMC article.
References
-
- Caux C, Dezutter-Dambuyant C, Schmitt D., and, Banchereau J. GM-CSF and TNF-alpha cooperate in the generation of dendritic Langerhans cells. Nature. 1992;360:258–261. - PubMed
-
- Katsafanas GC., and, Moss B. Vaccinia virus intermediate stage transcription is complemented by Ras-GTPase-activating protein SH3 domain-binding protein (G3BP) and cytoplasmic activation/proliferation-associated protein (p137) individually or as a heterodimer. J Biol Chem. 2004;279:52210–52217. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
