

Birth size distribution in 3,705 infants born to mothers with type 1 diabetes: a population-based study
- PMID: 21430084
- PMCID: PMC3114507
- DOI: 10.2337/dc10-2406
Birth size distribution in 3,705 infants born to mothers with type 1 diabetes: a population-based study
Abstract
Objective: To characterize birth size distribution in infants born to mothers with type 1 diabetes. In particular, the relationship between birth weight (BW) and length (BL) was studied because it may provide information on different causal pathways of fetal macrosomia commonly seen in diabetic pregnancies.
Research design and methods: This was a population-based cohort study of 3,705 infants of type 1 diabetic mothers (1,876 boys), with a gestational age of 28-43 weeks, born in Sweden between 1998 and 2007. BW and BL were retrieved from the Medical Birth Registry and expressed as SD scores (SDS). Ponderal index (PI) was calculated as BW in g/length in cm³. A BW >90th and a PI ≤ 90th percentile was defined as proportionate large-for-gestational age (LGA), whereas if both BW and PI > 90th percentile, the infant was categorized as disproportionately large. Values are mean (SD).
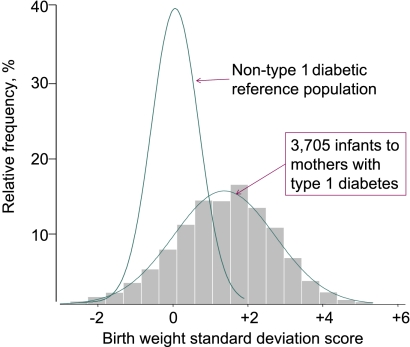
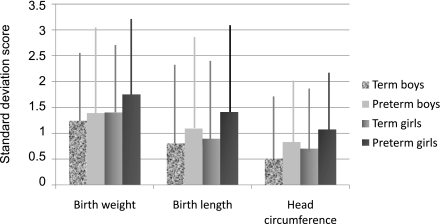
Results: The BW distribution for offspring of type 1 diabetic mothers was bell-shaped, significantly broader, and markedly shifted to the right (BWSDS: 1.27 [1.48]) of the reference. Of the infants born to diabetic mothers, 47% were LGA, and among them, 46% were disproportionately large compared with 35% in nondiabetic LGA infants (P < 0.001). Female offspring of type 1 diabetic mothers had significantly higher BWSDS than males (1.34 vs. 1.20, P < 0.01), and preterm infants had higher BWSDS than term infants (1.41 vs. 1.23, P < 0.01)
Conclusions: Fetal macrosomia in type 1 diabetic pregnancies is due to a right-shift and broadening of the entire BW distribution. The large number of disproportionate LGA infants born to type 1 diabetic mothers suggests an underlying metabolic problem. Fetal macrosomia was more pronounced in preterm and female offspring of type 1 diabetic mothers.
Figures
References
-
- Hanson U, Persson B. Outcome of pregnancies complicated by type 1 insulin-dependent diabetes in Sweden: acute pregnancy complications, neonatal mortality and morbidity. Am J Perinatol 1993;10:330–333 - PubMed
-
- Jensen DM, Damm P, Moelsted-Pedersen L, et al. Outcomes in type 1 diabetic pregnancies: a nationwide, population-based study. Diabetes Care 2004;27:2819–2823 - PubMed
-
- Lewis DF, Edwards MS, Asrat T, Adair CD, Brooks G, London SJ. Can shoulder dystocia be predicted? Preconceptive and prenatal factors. J Reprod Med 1998;43:654–658 - PubMed
-
- Berk MA, Mimouni F, Miodovnik M, Hertzberg V, Valuck J. Macrosomia in infants of insulin-dependent diabetic mothers. Pediatrics 1989;83:1029–1034 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
