

Socioeconomic status, Medicaid coverage, clinical comorbidity, and rehospitalization or death after an incident heart failure hospitalization: Atherosclerosis Risk in Communities cohort (1987 to 2004)
- PMID: 21430286
- PMCID: PMC3098576
- DOI: 10.1161/CIRCHEARTFAILURE.110.959031
Socioeconomic status, Medicaid coverage, clinical comorbidity, and rehospitalization or death after an incident heart failure hospitalization: Atherosclerosis Risk in Communities cohort (1987 to 2004)
Abstract
Background: Among patients with heart failure (HF), early readmission or death and repeat hospitalizations may be indicators of poor disease management or more severe disease.
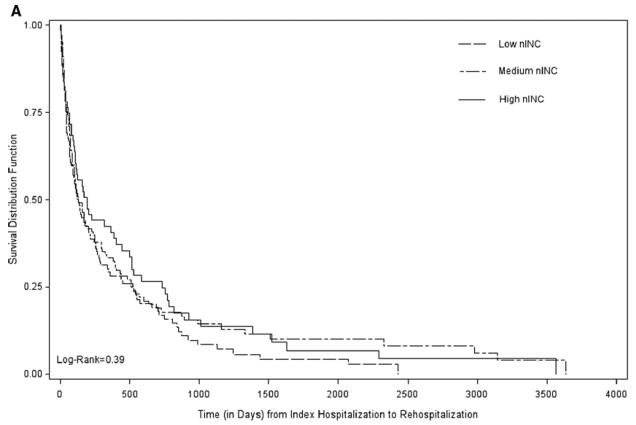
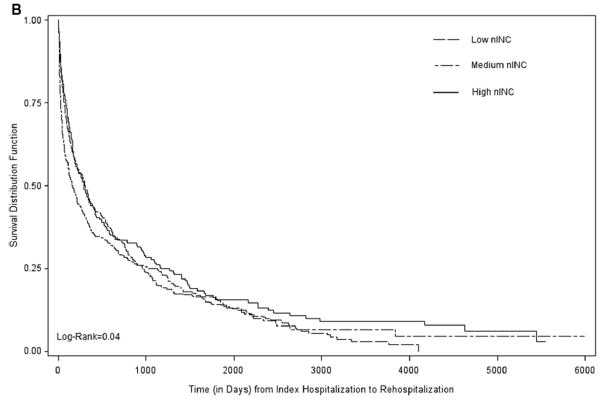
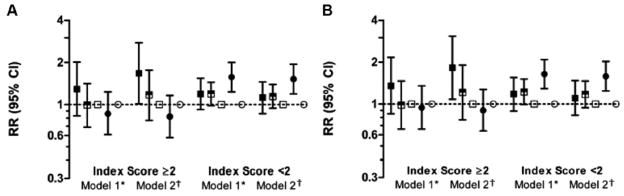
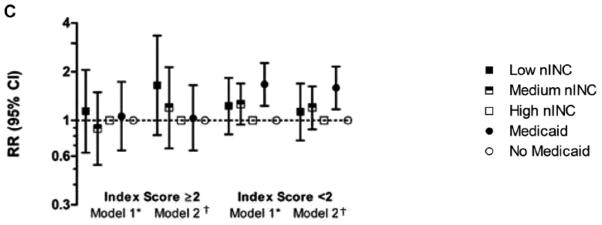
Methods and results: We assessed the association of neighborhood median household income (nINC) and Medicaid status with rehospitalization or death in the Atherosclerosis Risk in Communities cohort study (1987 to 2004) after an incident HF hospitalization in the context of individual socioeconomic status and evaluated the relationship for modification by demographic and comorbidity factors. We used generalized linear Poisson mixed models to estimate rehospitalization rate ratios and 95% CIs and Cox regression to estimate hazard ratios (HRs) and 95% CIs of rehospitalization or death. In models controlling for race and study community, sex, age at HF diagnosis, body mass index, hypertension, educational attainment, alcohol use, and smoking, patients with a high burden of comorbidity who were living in low-nINC areas at baseline had an elevated hazard of all-cause rehospitalization (HR, 1.40; 95% CI, 1.10 to 1.77), death (HR, 1.36; 95% CI, 1.02 to 1.80), and rehospitalization or death (HR, 1.36; 95% CI, 1.08 to 1.70) as well as increased rates of hospitalization compared to those with a high burden of comorbidity living in high-nINC areas. Medicaid recipients with a low level of comorbidity had an increased hazard of all-cause rehospitalization (HR, 1.19; 95% CI, 1.05 to 1.36) and rehospitalization or death (HR, 1.21; 95% CI, 1.07 to 1.37) and a higher rate of repeat hospitalizations compared to non-Medicaid recipients.
Conclusions: Comorbidity burden appears to influence the association among nINC, Medicaid status, and rehospitalization and death in patients with HF.
Figures

Comment in
-
The socio-geography of heart failure: why it matters.Circ Heart Fail. 2011 May;4(3):244-5. doi: 10.1161/CIRCHEARTFAILURE.111.962191. Circ Heart Fail. 2011. PMID: 21586735 No abstract available.
Similar articles
-
Hospital length of stay for incident heart failure: Atherosclerosis Risk in Communities (ARIC) cohort: 1987-2005.J Healthc Qual. 2014 Jan-Feb;36(1):45-51. doi: 10.1111/j.1945-1474.2012.00211.x. Epub 2012 Dec 3. J Healthc Qual. 2014. PMID: 23206293
-
Employment status at time of first hospitalization for heart failure is associated with a higher risk of death and rehospitalization for heart failure.Eur J Heart Fail. 2018 Feb;20(2):240-247. doi: 10.1002/ejhf.1046. Epub 2017 Nov 16. Eur J Heart Fail. 2018. PMID: 29148231
-
Burden and Timing of Hospitalizations in Heart Failure: A Community Study.Mayo Clin Proc. 2017 Feb;92(2):184-192. doi: 10.1016/j.mayocp.2016.11.009. Mayo Clin Proc. 2017. PMID: 28160871 Free PMC article.
-
Neighborhood socioeconomic status, Medicaid coverage and medical management of myocardial infarction: atherosclerosis risk in communities (ARIC) community surveillance.BMC Public Health. 2010 Oct 21;10:632. doi: 10.1186/1471-2458-10-632. BMC Public Health. 2010. PMID: 20964853 Free PMC article.
-
The association of lipoprotein(a) with incident heart failure hospitalization: Atherosclerosis Risk in Communities study.Atherosclerosis. 2017 Jul;262:131-137. doi: 10.1016/j.atherosclerosis.2017.05.014. Epub 2017 May 12. Atherosclerosis. 2017. PMID: 28554015 Free PMC article.
Cited by
-
Psychosocial Syndemics and Multimorbidity in Patients with Heart Failure †.J Psychiatr Brain Sci. 2021;6:e210006. doi: 10.20900/jpbs.20210006. Epub 2021 Apr 13. J Psychiatr Brain Sci. 2021. PMID: 33954261 Free PMC article.
-
Impact of Socioeconomic Status on Mortality and Readmission in Patients With Heart Failure With Reduced Ejection Fraction: The ARIC Study.J Am Heart Assoc. 2022 Sep 20;11(18):e024057. doi: 10.1161/JAHA.121.024057. Epub 2022 Sep 14. J Am Heart Assoc. 2022. PMID: 36102228 Free PMC article.
-
Racial Disparities in Access to High-Volume Mitral Valve Transcatheter Edge-to-Edge Repair Centers.J Soc Cardiovasc Angiogr Interv. 2022 Jul 13;1(5):100398. doi: 10.1016/j.jscai.2022.100398. eCollection 2022 Sep-Oct. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 39131452 Free PMC article.
-
Clinical adoption of prognostic biomarkers: the case for heart failure.Prog Cardiovasc Dis. 2012 Jul-Aug;55(1):3-13. doi: 10.1016/j.pcad.2012.05.004. Prog Cardiovasc Dis. 2012. PMID: 22824105 Free PMC article. Review.
-
Gender Differences in the Social Determinants of the Long-term Prognosis for Severely Decompensated Acute Heart Failure in Patients over 75 Years of Age.Intern Med. 2019 Oct 15;58(20):2931-2941. doi: 10.2169/internalmedicine.2757-19. Epub 2019 Jun 27. Intern Med. 2019. PMID: 31243215 Free PMC article.
References
-
- Heart Disease and Stroke Statistics - 2005 Update. Dallas, Texas: American Heart Association; 2005. pp. 1–63.
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Stafford R, Thom T, Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics--2010 Update: A Report From the American Heart Association. Circulation. 2010;121:e46–215. - PubMed
-
- MedPAC. Report to the Congress: Promoting Greater Efficiency in Medicare. Medicare Payment Advisory Commission (MedPAC); 2007.
-
- Schocken DD, Benjamin EJ, Fonarow GC, Krumholz HM, Levy D, Mensah GA, Narula J, Shor ES, Young JB, Hong Y. Prevention of Heart Failure. A Scientific Statement From the American Heart Association Councils on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular Nursing, and High Blood Pressure Research; Quality of Care and Outcomes Research Interdisciplinary Working Group; and Functional Genomics and Translational Biology Interdisciplinary Working Group. Circulation. 2008;117:2544–65. - PubMed
-
- Fang J, Mensah GA, Croft JB, Keenan NL. Heart Failure-Related Hospitalization in the U.S., 1979 to 2004. Journal of the American College of Cardiology. 2008;52:428–434. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC055019/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- N01 HC055015/HL/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- T32 HL007055/HL/NHLBI NIH HHS/United States
- 5-T32-HL007055/HL/NHLBI NIH HHS/United States
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- R24 HD050924/HD/NICHD NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
