

Direct repair of lumbar spondylolysis by Buck's technique
- PMID: 21430868
- PMCID: PMC3051120
- DOI: 10.4103/0019-5413.77133
Direct repair of lumbar spondylolysis by Buck's technique
Abstract
Background: The lesion in spondylolysis is a nonunion that follows a fatigue fracture of pars interarticularis. Direct repair of the pars defect is a logical alternative to fusion as it helps to preserve the motion segment and prevents abnormal stresses at the adjacent levels. The purpose of the study is to analyze the clinical and radiological results of direct screw osteosynthesis of the pars defect by the Buck's method in patients with symptomatic spondylolysis with or without grade 1 spondylolisthesis.
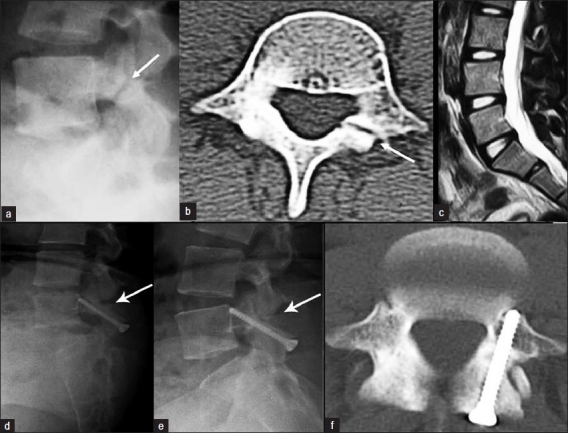
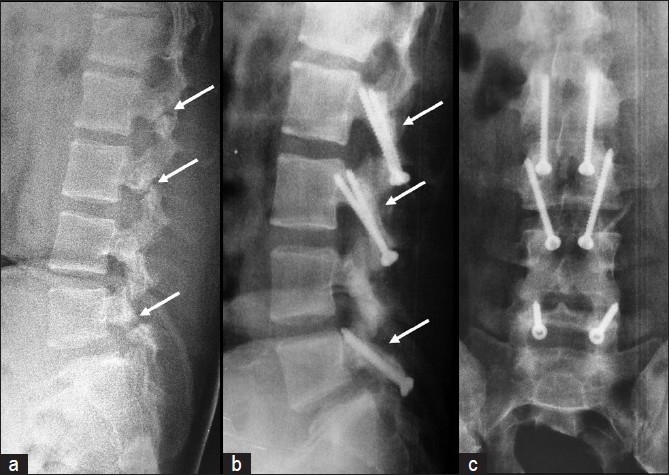
Materials and methods: Nine patients (six males, three females, mean age 24 years) with symptomatic spondylolysis with or without grade 1 spondylolisthesis and a normal disc in magnetic resonance imaging (MRI), who failed conservative treatment, underwent surgery between January 2000 and April 2009. Of them five patients had bilateral lysis at one level, one had bilateral lysis at three levels and two levels each and two had unilateral lysis at one level. Direct pars repair by the Buck's method with internal fixation of the defect using 4.5 mm cortical screws and cancellous bone grafting was done. The mean follow-up period was 45 months. MacNab criteria were used to evaluate the postoperative functional outcome. Healing of the pars defect was assessed by plain radiographs and computed tomography (CT) scan.
Results: Spondylolysis was bilateral in seven and unilateral in two patients. Two patients had associated grade 1 spondylolisthesis. The mean operative time was 58 minutes (range 45 - 75 minutes) and blood loss was 98 ml (50 - 140 ml). Although radiological fusion was observed in all patients at a mean follow-up of 45 months (range 9 to 108 months), the functional outcome was excellent in two patients and good in five, with one fair and one poor result. The overall result of the procedure was satisfactory in 78% (7/9) of the patients. The two patients with associated grade 1 spondylolisthesis had fair and poor results. No complications were encountered in the perioperative or postoperative period.
Conclusions: In carefully selected patients, direct repair of the pars defect by the Buck's technique of internal fixation and bone grafting was a safe and effective alternative to fusion in younger patients with symptomatic spondylolysis, without associated spondylolisthesis, who failed conservative management.
Keywords: Buck’s technique; direct pars repair; pars interarticularis; spondylolysis.
Conflict of interest statement
Figures

Similar articles
-
Lumbar spondylolysis - Current concepts review.J Clin Orthop Trauma. 2021 Jul 30;21:101535. doi: 10.1016/j.jcot.2021.101535. eCollection 2021 Oct. J Clin Orthop Trauma. 2021. PMID: 34405089 Free PMC article. Review.
-
Direct Repair of the Pars Interarticularis Defect in Spondylolysis.J Spinal Disord Tech. 2012 Aug 29. doi: 10.1097/BSD.0b013e31827069e4. Online ahead of print. J Spinal Disord Tech. 2012. PMID: 22935714
-
Lumbo-sacral motion conserved after isthmic reconstruction: long-term results.J Child Orthop. 2014 Feb;8(1):97-103. doi: 10.1007/s11832-014-0560-9. Epub 2014 Jan 29. J Child Orthop. 2014. PMID: 24488849 Free PMC article.
-
Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis.Spine (Phila Pa 1976). 2007 Apr 20;32(9):995-1000. doi: 10.1097/01.brs.0000260978.10073.90. Spine (Phila Pa 1976). 2007. PMID: 17450075 Clinical Trial.
-
Is there a place for surgical repair in adults with spondylolysis or grade-I spondylolisthesis-a systematic review and treatment algorithm.Spine J. 2021 Aug;21(8):1268-1285. doi: 10.1016/j.spinee.2021.03.011. Epub 2021 Mar 21. Spine J. 2021. PMID: 33757872
Cited by
-
A Review of Treatment for Acute and Chronic Pars Fractures in the Lumbar Spine.Curr Rev Musculoskelet Med. 2022 Aug;15(4):259-271. doi: 10.1007/s12178-022-09760-9. Epub 2022 May 2. Curr Rev Musculoskelet Med. 2022. PMID: 35499747 Free PMC article. Review.
-
Lumbar spondylolysis - Current concepts review.J Clin Orthop Trauma. 2021 Jul 30;21:101535. doi: 10.1016/j.jcot.2021.101535. eCollection 2021 Oct. J Clin Orthop Trauma. 2021. PMID: 34405089 Free PMC article. Review.
-
Retrospective Comparative Study of Pedicle Screw Fixation via Quadrant Retractor and Buck's Technique in the Treatment of Adolescent Spondylolysis.Orthop Surg. 2022 Jan;14(1):111-118. doi: 10.1111/os.13165. Epub 2021 Dec 8. Orthop Surg. 2022. PMID: 34881509 Free PMC article.
-
Minimally invasive direct repair of bilateral lumbar spine pars defects in athletes.Case Rep Med. 2013;2013:659078. doi: 10.1155/2013/659078. Epub 2013 Apr 30. Case Rep Med. 2013. PMID: 23737800 Free PMC article.
-
Minimally-Invasive versus Conventional Repair of Spondylolysis in Athletes: A Review of Outcomes and Return to Play.Asian Spine J. 2017 Oct;11(5):832-842. doi: 10.4184/asj.2017.11.5.832. Epub 2017 Oct 11. Asian Spine J. 2017. PMID: 29093794 Free PMC article. Review.
References
-
- Wiltse LL, Widell EH, Jr, Jackson DW. Fatigue fracture: The basic lesion in isthmic spondylolisthesis. J Bone Joint Surg Am. 1975;57-A:17–22. - PubMed
-
- Buck JE. Direct repair of the defect in spondylolisthesis. Preliminary report. J Bone Joint Surg. 1970;52-B:432–7. - PubMed
-
- Hensinger RN. Spondylolysis and spondylolisthesis in children and adolescents: Current concepts review. J Bone Joint Surg Am. 1989;71:1098–107. - PubMed
-
- Fredrickson BE, Baker D, McHolick WJ, Yuan HA, Lubicky JP. The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am. 1984;66:699–707. - PubMed
-
- Bradford DS. Management of spondylolysis and spondylolisthesis. Instr Course Lect. 1983;32:151–62. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous