

doi: 10.4103/0971-3026.76061.
Pictorial essay: Complications of a swallowed fish bone
Affiliations
- PMID: 21431037
- PMCID: PMC3056375
- DOI: 10.4103/0971-3026.76061
Item in Clipboard
Pictorial essay: Complications of a swallowed fish bone
Indian J Radiol Imaging.
2011 Jan.
Abstract
Unintentional ingestion of a fishbone (FB) is common, especially in populations with a high consumption of seafood. In most instances, the ingested FB passes uneventfully through the gastrointestinal (GI) tract, usually within a week. However, in certain cases, the FB may become impacted and lead to complications. Awareness of these complications is important as patients usually present with nonspecific symptoms and could be unaware of having ingested an FB.
Keywords: Abscess; bowel; fishbone; perforation.
Conflict of interest statement
Figures

Noncontrast coronal reformations (A,B) through the neck show a curvilinear FB extending from the region of the left tonsillar fossa into the parapharyngeal space (white arrows). There is associated surrounding soft tissue inflammatory thickening (black asterisk). A few small surrounding lymph nodes are also seen (black arrows in B).

Lateral radiograph of the neck of an elderly patient shows a linear FB within the hypopharynx at the C5-6 level (black arrow). No evidence is seen of any thickening of the prevertebral soft tissues or cervical emphysema

Lateral radiograph of a patient shows widening of the prevertebral space, with small air locules within (arrow), findings consistent with a retropharyngeal abscess. A noncontrast CT scan (not shown) revealed the presence of an underlying FB, which is obscured on the radiograph by the surrounding soft tissue

Noncontrast axial CT scans show a curvilinear FB (black arrow in A) at the level of the cricopharyngeus. There is perforation of the pharyngeal wall on the left side with a small parapharyngeal abscess (white arrow in B)

Noncontrast axial CT scan shows a linear radiodense FB (white arrow) in the upper dorsal esophagus. Note that laterally the FB is seen to extend into the wall of the esophagus. On endoscopy, it was found to be partially embedded within the wall of esophagus, with the presence of a small tear
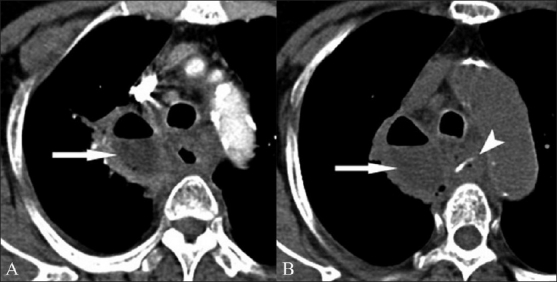
Contrast-enhanced (A) and noncontrast (B) axial CT scans show a large mediastinal abscess (arrows in both A and B) in the right paratracheal region, with associated stranding of the surrounding mediastinal fat. The esophageal wall is thickened. A linear FB (arrowhead in B) is seen within the lumen of the esophagus at the level of the arch of the esophagus

Coronal (A) and axial (B) noncontrast CT scans show a curvilinear FB at the level of the aortic arch (arrow). This is the second most common site of FB impaction within the esophagus. Note the close proximity to the aortic lumen which would partly explain the high incidence of vascular injuries within the mediastinum

Sequential axial contrast-enhanced CT scans through the lower abdomen show a linear radiodense FB (arrow) in the distal ileum. It can be seen to traverse the thickened bowel wall. Surrounding stranding of the mesenteric fat is noted. There was no pneumoperitoneum

Axial contrast-enhanced CT scans show focal fat stranding and localized pneumoperitoneum in relation to the ileal loops (white arrow in A). There is associated dilatation of the bowel loops, suggesting obstruction. The FB is seen distally in the large bowel (black arrow in B), reemphasizing the importance of closely scrutinizing the bowel loops distal to the inflamed segments

Small bowel perforation without obstruction. Axial (A) and coronal (B) contrast-enhanced CT scans show localized pneumoperitoneum and fat stranding in relation to focally thickened distal ileal loops (black arrows in A). The FB however, has since passed distally into the large bowel and can be easily overlooked on the axial images (white arrow in A). Note that the FB is fairly conspicuous on the coronal images (white arrow in B)

Axial (A) contrast-enhanced CT scan shows a small hyperdensity, which may be easily overlooked or confused with a vessel (black arrow in A), which however is very well appreciated in the sagittal reformatted image (arrow in B) penetrating through the bowel wall. Associated segmental bowel wall thickening is seen with presence of a small loculated collection (asterisk in B)

Non-contrast axial (A,B) CT scans show a questionable hyperdensity within the esophageal lumen, at the level of the thoracic inlet (arrows). The coronal reconstructed image however clearly shows the presence of a fine linear FB (arrow in C). Coronal images are in general more useful in cases of FB since the bone is usually oriented orthogonally to the acquired axial images
References
-
- Goh BK, Tan YM, Lin SE, Chow PK, Cheah FK, Ooi LL, et al. CT in the preoperative diagnosis of fish bone perforation of the gastrointestinal tract. AJR Am J Roentgenol. 2006;187:710–4. - PubMed
-
- Coulier B, Tancredi MH, Ramboux A. Spiral CT and multidetector-row CT diagnosis of perforation of the small intestine caused by ingested foreign bodies. Eur Radiol. 2004;14:1918–25. - PubMed
-
- Zissin R, Osadchy A, Gayer G. Abdominal CT findings in small bowel perforation. Br J Radiol. 2009;82:162–71. - PubMed
-
- Brandão D, Canedo A, Maia M, Ferreira J, Vaz G. Duodenocaval fistula as a result of a fish bone perforation. J Vasc Surg. 2010;51:1276–8. - PubMed
-
- Foo TH. Migratory fish bone in the thyroid gland. Singapore Med J. 1993;34:142–4. - PubMed
LinkOut - more resources
Full Text Sources