

Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
- PMID: 21432843
- PMCID: PMC3155861
- DOI: 10.1002/cncr.26070
Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
Abstract
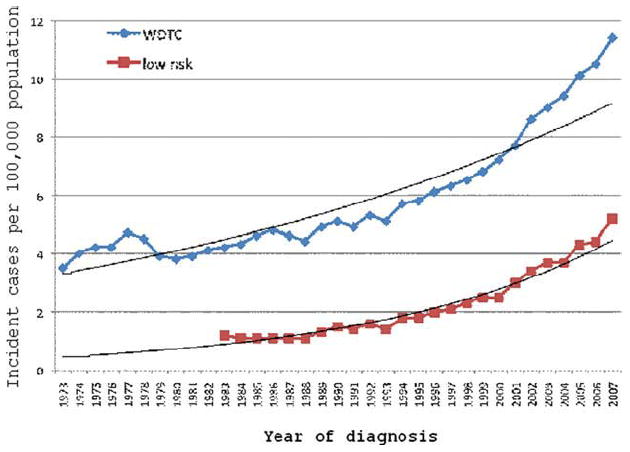
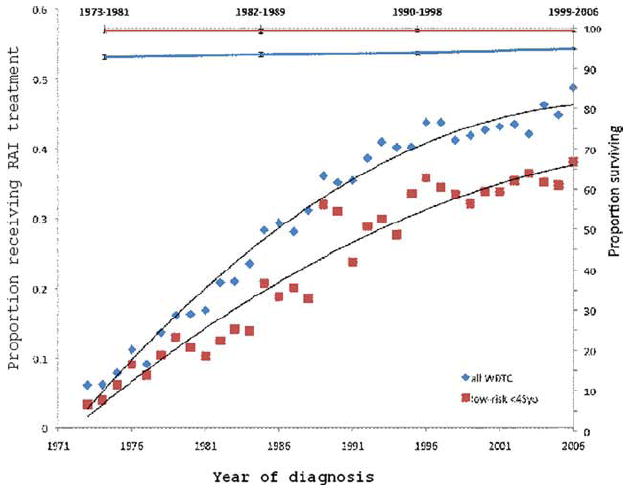
Background: American Thyroid Association guidelines currently recommend the selective use of radioactive iodine (RAI) therapy in patients with well differentiated thyroid cancer (WDTC). Despite these guidelines, RAI ablation has been used routinely in all but the very lowest risk patients with thyroid cancer over the last 30 years. The objective of this study was to evaluate patterns of RAI use and elevated risk of secondary primary malignancies (SPM) in patients with low-risk (T1N0) WDTC.
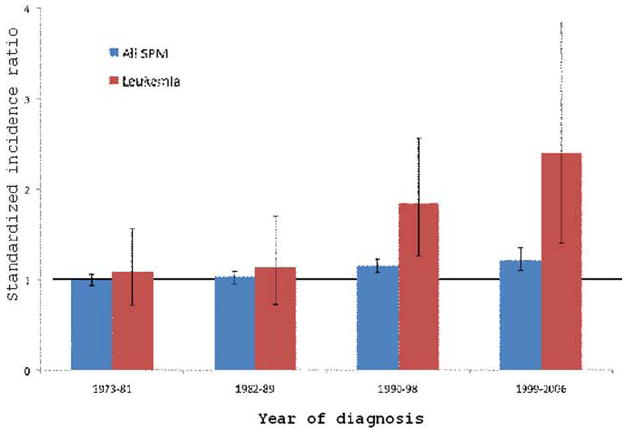
Methods: The Surveillance, Epidemiology, and End Results (SEER) database was used to analyze trends in RAI use over time in the United States. To determine the excess risk of SPM, the standardized incidence ratio (SIR) and excess absolute risk (EAR) of various cancers were calculated in the 2 cohorts. Between 1973 and 2007, 37,176 patients with WDTC were followed in the SEER Program, equating to 408,750 person-years at risk (PYR). In total, 14,589 patients received RAI, and SPMs were observed in 3223 patients.
Results: During the study period, the rate of RAI use in patients with low-risk (T1N0) WDTC increased from 3.3% to 38.1%. For low-risk patients, the SIR of SPM was 1.21 (95% confidence interval [CI], 0.93-1.54), and the EAR was 4.6 excess cases per 10,000 PYR. SPM with significantly elevated risk because of RAI were salivary gland malignancies (SIR = 11.13; 95% CI, 1.35-40.2) and leukemia (SIR = 5.68; 95% CI, 2.09-12.37). The excess risk of leukemia was significantly greater in patients aged <45 years (SIR = 5.32; 95% CI, 2.75-9.30) compared with the excess risk in older patients (SIR = 2.26; 95% CI, 1.43-3.39).
Conclusions: The increased risk of a SPM in patients with low-risk (T1N0) WDTC, along with a lack of data demonstrating improved survival outcomes with adjuvant RAI, provide a compelling argument in favor of rationing the use of RAI in this patient population.
Copyright © 2011 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES The authors made no disclosures.
Figures
References
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006;295:2164–2167. - PubMed
-
- Iyer NG, Shaha AR, Silver CE, et al. Thyroid incidentalomas: to treat or not to treat. Eur Arch Otorhinolaryngol. 2010;267:1019–1026. - PubMed
-
- Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998;338:297–306. - PubMed
-
- Tuttle RM, Leboeuf R, Shaha AR. Medical management of thyroid cancer: a risk adapted approach. J Surg Oncol. 2008;97:712–716. - PubMed
-
- Hay ID, Thompson GB, Grant CS, et al. Papillary thyroid carcinoma managed at the Mayo Clinic during 6 decades (1940-1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg. 2002;26:879–885. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
