

Management of tinea capitis in childhood
- PMID: 21437064
- PMCID: PMC3047946
- DOI: 10.2147/ccid.s7992
Management of tinea capitis in childhood
Abstract
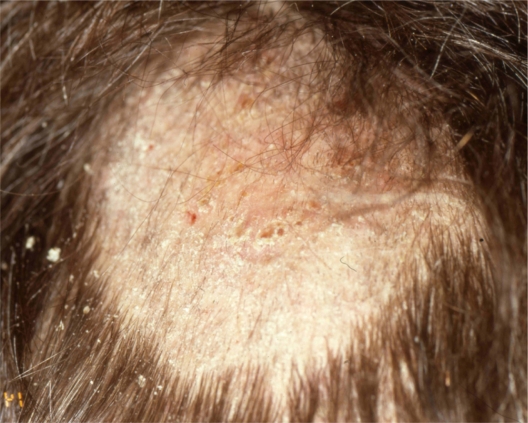
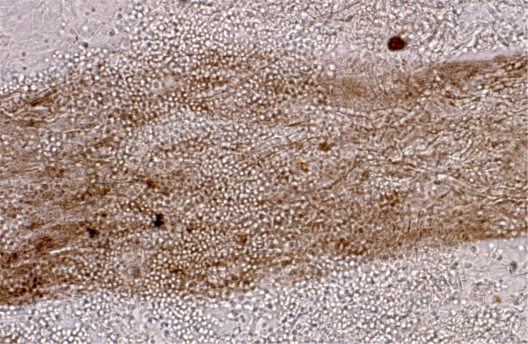
Tinea capitis (TC) is a common dermatophyte infection affecting primarily prepubertal children. The causative pathogens belong to only two genera: Trichophyton and Microsporum. Although there is a great local variation in the epidemiology of TC worldwide, T. tonsurans is currently the most common cause of TC with M. canis second. Even though there is an emerging number of anthropophilic scalp infections, M. canis remains the predominant causative organism in many countries of the Mediterranean basin, the most important dermatophyte carriers being stray cats and dogs as well as pet puppies, kittens and rabbits. TC always requires systemic treatment because topical antifungal agents do not penetrate down to the deepest part of the hair follicle. Since the late 1950s, griseofulvin has been the gold standard for systemic therapy of TC. It is active against dermatophytes and has a long-term safety profile. The main disadvantage of griseofulvin is the long duration of treatment required which may lead to reduced compliance. The newer oral antifungal agents including terbinafine, itraconazole, ketokonazole, and fluconazole appear to have efficacy rates and potential adverse effects similar to those of griseofulvin in children with TC caused by Trichophyton species, while requiring a much shorter duration of treatment. They may, however, be more expensive.
Keywords: children; fluconazole; fungal infection; greseofulvin; itraconazole; pediatric infection; terbinafine; tinea capitis; treatment.
Figures


References
-
- Gupta AK, Summerbell RC. Tinea capitis. Med Mycol. 2000;38:255–287. - PubMed
-
- Elewski B. Tinea capitis: a current perspective. J Am Acad Dermatol. 2000;42:1–20. - PubMed
-
- Ilkit M, Demirhindi H. Asymptomatic dermatophyte scalp carriage: laboratory diagnosis, epidemiology and management. Mycopathologia. 2008;165:61–71. - PubMed
-
- Razzaq Adel AA, Sultan AO, Basmiah AM, Aftab A, Nabel N. Prevalence of tinea capitis in southern Kuwait. Mycoses. 2007;50:317–320. - PubMed
-
- Romano C, Gianni C, Papini M. Tinea capitis in infants less than 1 year of age. Pediatr Dermatol. 2001;18:465–468. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
