

Cardioprotection conferred by exercise training is blunted by blockade of the opioid system
- PMID: 21437452
- PMCID: PMC3044560
- DOI: 10.1590/s1807-59322011000100026
Cardioprotection conferred by exercise training is blunted by blockade of the opioid system
Abstract
Objectives: To investigate the effect of opioid receptor blockade on the myocardial protection conferred by chronic exercise and to compare exercise training with different strategies of myocardial protection (opioid infusion and brief periods of ischemia-reperfusion) preceding irreversible left anterior descending coronary ligation.
Introduction: The acute cardioprotective effects of exercise training are at least partly mediated through opioid receptor-dependent mechanisms in ischemia-reperfusion models.
Methods: Male Wistar rats (n = 76) were randomly assigned to 7 groups: (1) control; (2) exercise training; (3) morphine; (4) intermittent ischemia-reperfusion (three alternating periods of left anterior descending coronary occlusion and reperfusion); (5) exercise training+morphine; (6) naloxone (a non-selective opioid receptor blocker) plus morphine; (7) naloxone before each exercise-training session. Myocardial infarction was established in all groups by left anterior descending coronary ligation. Exercise training was performed on a treadmill for 60 minutes, 5 times/week, for 12 weeks, at 60% peak oxygen (peak VO₂). Infarct size was histologically evaluated.
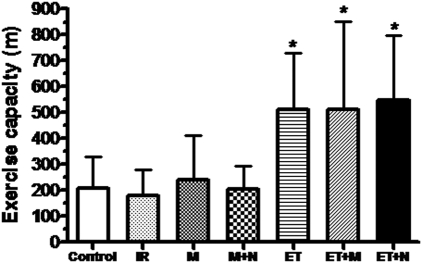
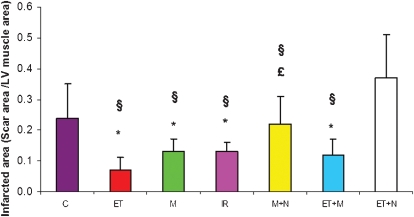
Results: Exercise training significantly increased exercise capacity and ΔVO2 (VO₂ peak - VO₂ rest) (p < 0.01 vs. sedentary groups). Compared with control, all treatment groups except morphine plus naloxone and exercise training plus naloxone showed a smaller infarcted area (p < 0.05). No additional decrease in infarct size occurred in the exercise training plus morphine group. No difference in myocardial capillary density (p = 0.88) was observed in any group.
Conclusions: Exercise training, morphine, exercise training plus morphine and ischemia-reperfusion groups had a smaller infarcted area than the control group. The effect of chronic exercise training in decreasing infarct size seems to occur, at least in part, through the opioid receptor stimulus and not by increasing myocardial perfusion.
Figures
References
-
- Dickson EW, Hogrefe CP, Ludwig PS, Ackermann LW, Stoll LL, Denning GM. Exercise enhances myocardial ischemic tolerance via an opioid receptor-dependent mechanism. Am J Physiol Heart Circ Physiol. 2008;294:H402–8. 10.1152/ajpheart.00280.2007 - DOI - PubMed
-
- Hull SS, Jr, Vanoli E, Adamson PB, Verrier RL, Foreman RD, Schwartz PJ. Exercise training confers anticipatory protection from sudden death during acute myocardial ischemia. Circulation. 1994;89:548–52. - PubMed
-
- Morris JN, Everitt MG, Pollard R, Chave SP, Semmence AM. Vigorous exercise in leisure-time: protection against coronary heart disease. Lancet. 1980;2:1207–10. 10.1016/S0140-6736(80)92476-9 - DOI - PubMed
-
- White FC, Bloor CM, Mckirnan MD, Carroll SM. Exercise training in swine promotes growth of arteriolar bed and capillary angiogenesis in heart. J Appl Physiol. 1998;85:1160–8. - PubMed
-
- Marcil M, Bourduas K, Ascah A, Burelle Y. Exercise training induces respiratory substrate-specific decrease in Ca2+-induced permeability transition pore opening in heart mitochondria. Am J Physiol Heart Circ Physiol. 2006;290:H1549–57. 10.1152/ajpheart.00913.2005 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
