

Collaterals dramatically alter stroke risk in intracranial atherosclerosis
- PMID: 21437932
- PMCID: PMC3117968
- DOI: 10.1002/ana.22354
Collaterals dramatically alter stroke risk in intracranial atherosclerosis
Abstract
Objective: Stroke risk due to intracranial atherosclerosis increases with degree of arterial stenosis. We evaluated the previously unexplored role of collaterals in modifying stroke risk in intracranial atherosclerosis and impact on subsequent stroke characteristics.
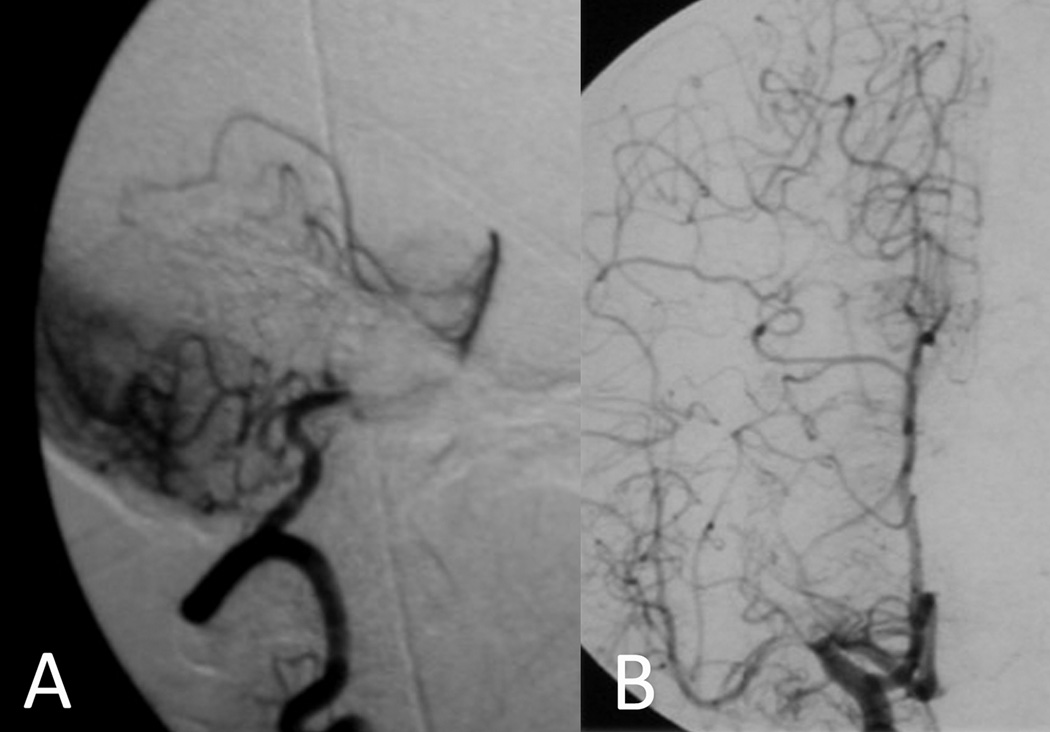
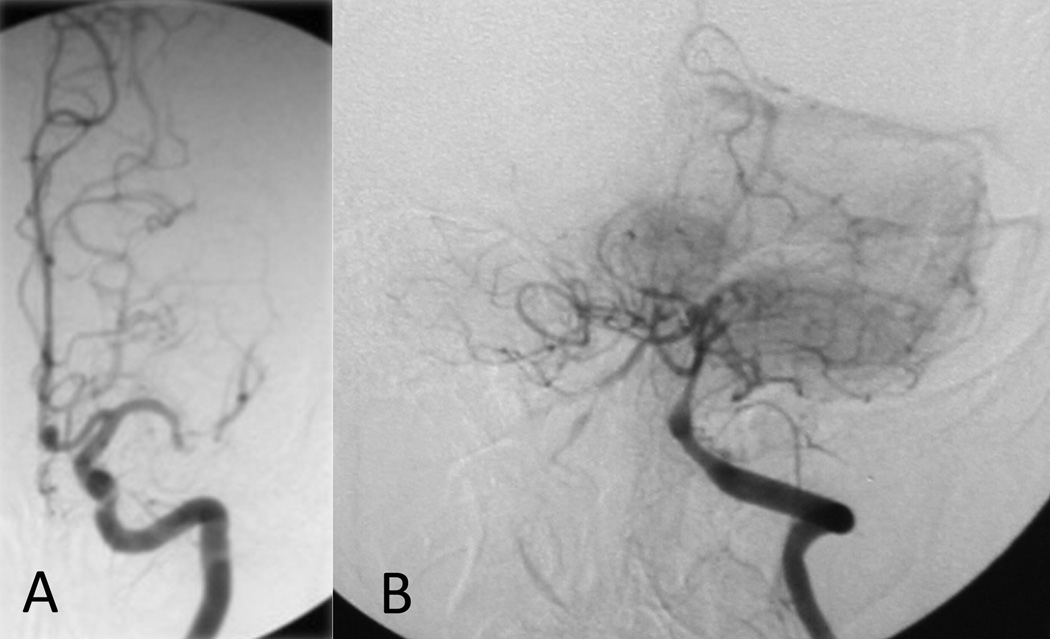
Methods: Collateral flow was graded in blind fashion on 287 of 569 baseline angiograms (stenoses of 50-99% and adequate collateral views) in the Warfarin--Aspirin Symptomatic Intracranial Disease (WASID) trial. Statistical models predicted stroke in the symptomatic arterial territory based on collateral flow grade, percentage of stenosis, and previously demonstrated independent covariates.
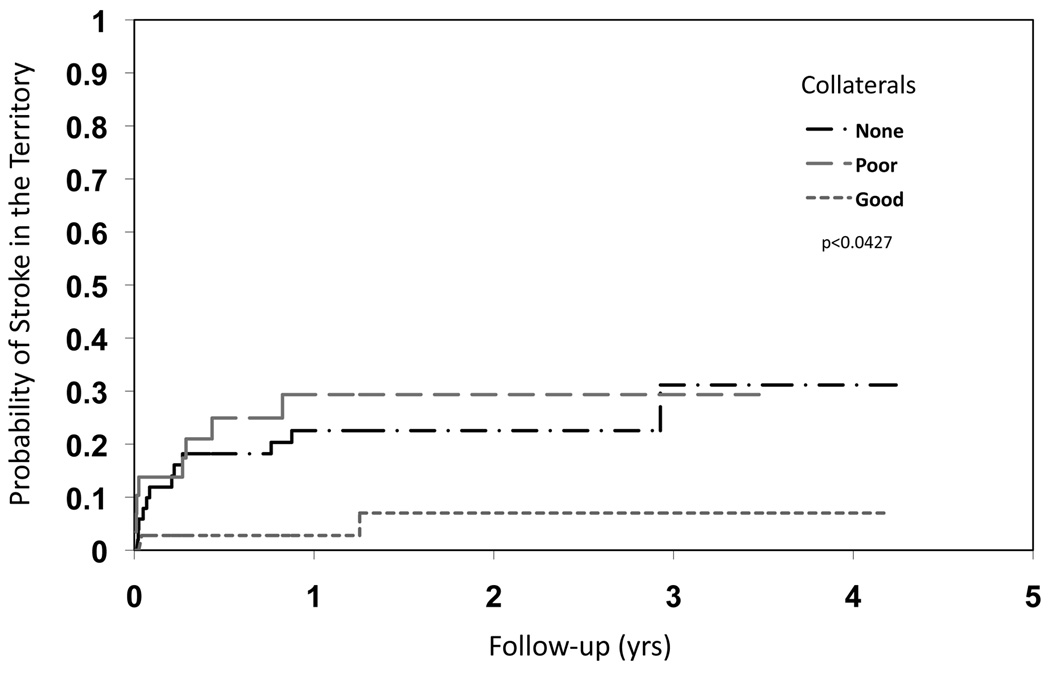
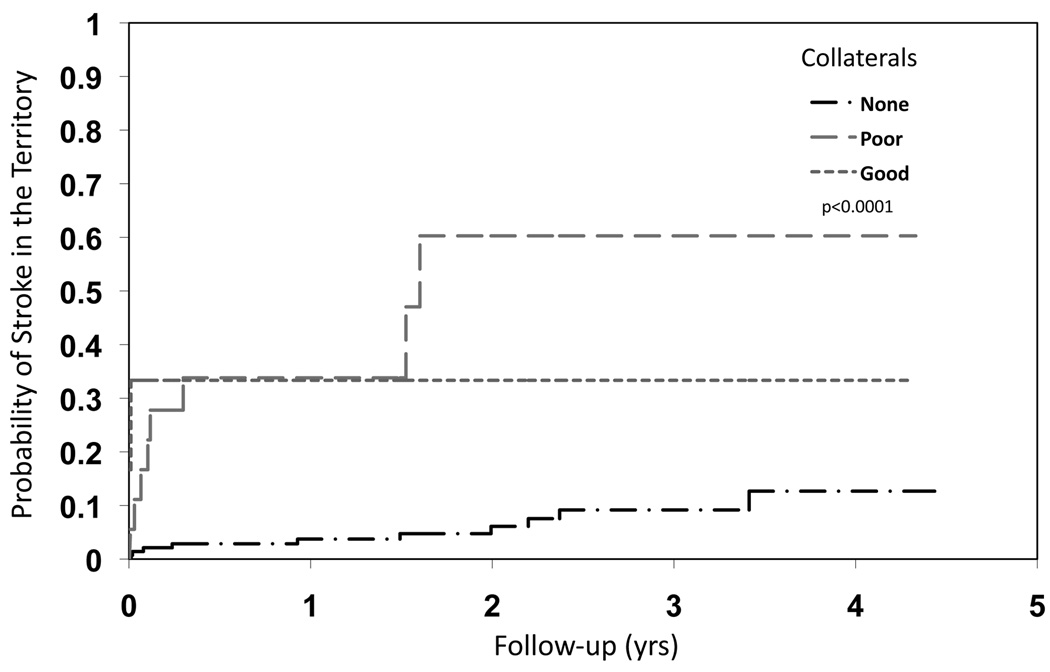
Results: Across all stenoses, extent of collaterals was a predictor for subsequent stroke in the symptomatic arterial territory (hazard ratio [HR] none vs good, 1.14; 95% confidence interval [CI], 0.39-3.30; poor vs good, 4.36; 95% CI, 1.46-13.07; p < 0.0001). For 70 to 99% stenoses, more extensive collaterals diminished risk of subsequent territorial stroke (HR none vs good, 4.60; 95% CI, 1.03-20.56; poor vs good, 5.90; 95% CI, 1.25-27.81; p = 0.0427). At milder degrees of stenoses (50-69%), presence of collaterals was associated with greater likelihood of subsequent stroke (HR none vs good, 0.18; 95% CI, 0.04-0.82; poor vs good, 1.78; 95% CI, 0.37-8.57; p < 0.0001). In multivariate analyses, extent of collaterals was an independent predictor for subsequent stroke in the symptomatic arterial territory (HR none vs good, 1.62; 95% CI, 0.52-5.11; poor vs good, 4.78; 95% CI, 1.55-14.7; p = 0.0019).
Interpretation: Collateral circulation is a potent determinant of stroke risk in intracranial atherosclerosis, demonstrating a protective role with severe stenoses and identifying more unstable milder stenoses.
Copyright © 2011 American Neurological Association.
Figures
References
-
- Gorelick PB, Wong KS, Bae HJ, Pandey DK. Large artery intracranial occlusive disease: a large worldwide burden but a relatively neglected frontier. Stroke. 2008;39:2396–2399. - PubMed
-
- Wong LK. Global burden of intracranial atherosclerosis. Int J Stroke. 2006;1:158–159. - PubMed
-
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005;352:1305–1316. - PubMed
-
- Van Meurs KP, Wright LL, Ehrenkranz RA, et al. Inhaled nitric oxide for premature infants with severe respiratory failure. N Engl J Med. 2005;353:13–22. - PubMed
-
- Chimowitz MI, Kokkinos J, Strong J, et al. The Warfarin-Aspirin Symptomatic Intracranial Disease Study. Neurology. 1995;45:1488–1493. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 NS051688/NS/NINDS NIH HHS/United States
- 5M01 RR000750-32/RR/NCRR NIH HHS/United States
- U01 NS058728/NS/NINDS NIH HHS/United States
- K23NS054084/NS/NINDS NIH HHS/United States
- P50NS044378/NS/NINDS NIH HHS/United States
- M01 RR165001/RR/NCRR NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- M01 RR000425/RR/NCRR NIH HHS/United States
- P50 NS044378/NS/NINDS NIH HHS/United States
- 1R01 NS36643/NS/NINDS NIH HHS/United States
- K23 NS054084/NS/NINDS NIH HHS/United States
- R01 NS036643/NS/NINDS NIH HHS/United States
- M01 RR00425/RR/NCRR NIH HHS/United States
- M01 RR00039/RR/NCRR NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- 5M01 RR00080/RR/NCRR NIH HHS/United States
- M01 RR000083/RR/NCRR NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- M01 RR00083-42/RR/NCRR NIH HHS/United States
- K24 NS050307/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
