

Normal response to vaccines in inflammatory bowel disease patients treated with thiopurines
- PMID: 21438101
- PMCID: PMC3919517
- DOI: 10.1002/ibd.21688
Normal response to vaccines in inflammatory bowel disease patients treated with thiopurines
Abstract
Background: Thiopurines are considered immunosuppressive agents and may be associated with an increased risk for infections. However, few inflammatory bowel disease (IBD) patients are appropriately vaccinated, and data on their ability to mount an immune response are vague. We evaluated the effects of the thiopurines, azathioprine (AZA) and 6-mercaptopurine (6-MP), on cellular and humoral immune responses in IBD patients.
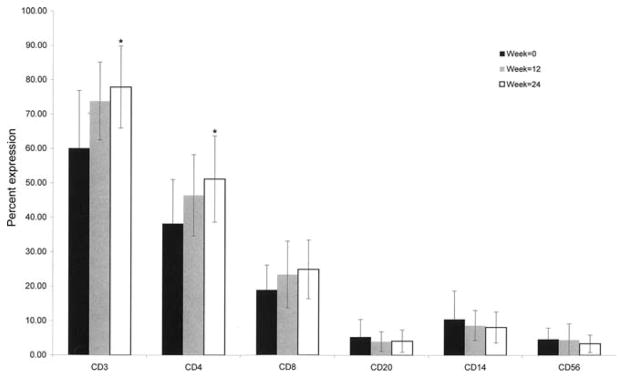
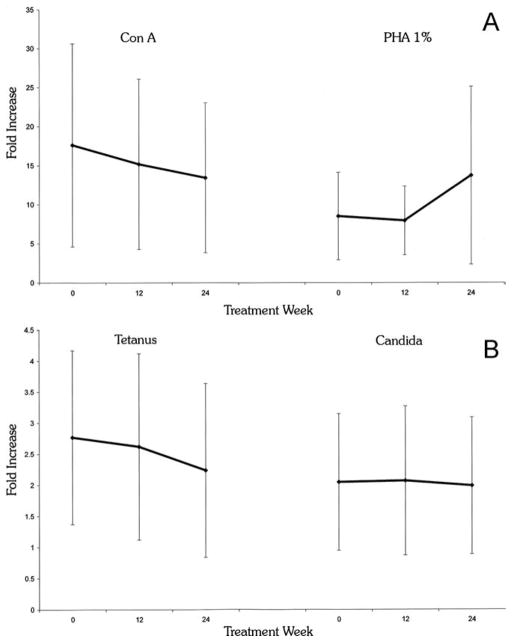
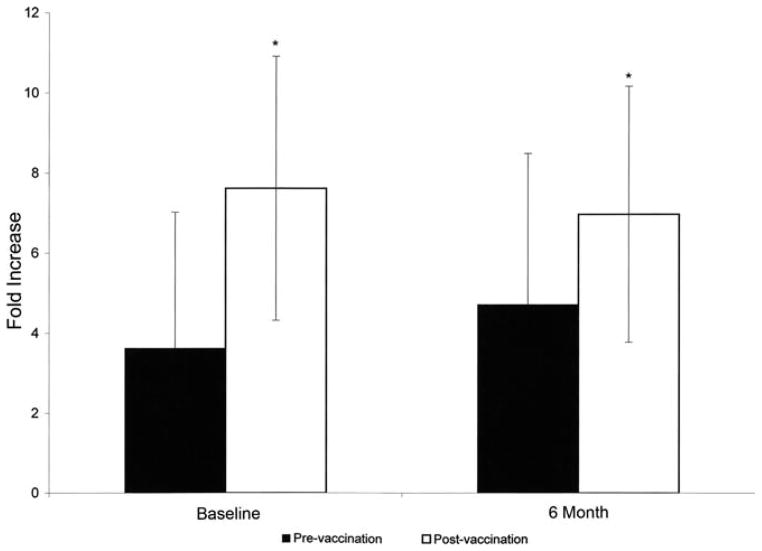
Methods: A prospective clinical investigation was conducted on IBD patients referred for thiopurine treatment. Immune competence was evaluated by assessing lymphocyte counts and phenotype, response to mitogen and antigen stimulation, immunoglobulin levels, and response to pneumococcal and tetanus vaccines (before treatment, week 0), and to Haemophilus influenza type b vaccine (at week 24).
Results: Thirty-one Crohn's disease and 12 ulcerative colitis patients who completed at least 24 weeks of therapy were included. The posttherapy average 6-MP dose was 1.05 ± 0.30 mg/kg, and white blood cell counts had decreased significantly from baseline values (P < 0.002). The posttreatment response to mitogens and antigens and the immunoglobulin levels were unchanged. Responses to vaccines were normal both in thiopurine-naïve and thiopurine-treated patients, suggesting that these patients were immunologically intact while on thiopurine therapy and capable of generating normal immune responses in vivo.
Conclusions: There is no evidence for any intrinsic systemic immunodeficiency in IBD patients. Thiopurines at the doses used for treating IBD showed no significant suppressive effect on the systemic cellular and humoral immune responses evaluated. Thiopurine-treated IBD patients can be safely and efficiently vaccinated.
Copyright © 2011 Crohn's & Colitis Foundation of America, Inc.
Figures
References
-
- Present DH, Korelitz BI, Wisch N, et al. Treatment of Crohn’s disease with 6-mercaptopurine. A long-term, randomized, double-blind study. N Engl J Med. 1980;302:981–987. - PubMed
-
- Prefontaine E, Sutherland LR, Macdonald JK, et al. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev. 2009;1:CD000067. - PubMed
-
- Shaye OA, Yadegari M, Abreu MT, et al. Hepatotoxicity of 6-mercaptopurine (6-MP) and azathioprine (AZA) in adult IBD patients. Am J Gastroenterol. 2007;102:2488–2494. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical