

Prolonged mechanical ventilation in critically ill patients: epidemiology, outcomes and modelling the potential cost consequences of establishing a regional weaning unit
- PMID: 21439086
- PMCID: PMC3219374
- DOI: 10.1186/cc10117
Prolonged mechanical ventilation in critically ill patients: epidemiology, outcomes and modelling the potential cost consequences of establishing a regional weaning unit
Abstract
Introduction: The number of patients requiring prolonged mechanical ventilation (PMV) is likely to increase. Transferring patients to specialised weaning units may improve outcomes and reduce costs. The aim of this study was to establish the incidence and outcomes of PMV in a UK administrative health care region without a dedicated weaning unit, and model the potential impact of establishing a dedicated weaning unit.
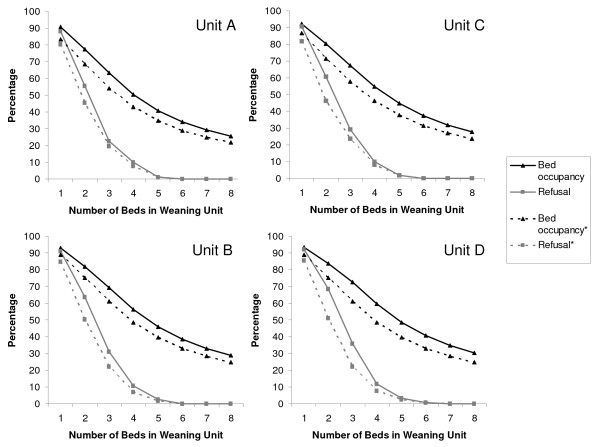
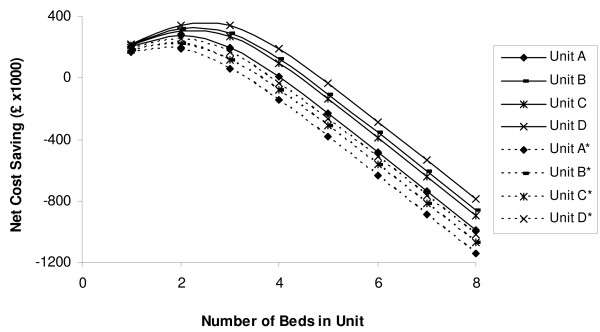
Methods: A retrospective cohort study was undertaken using a database of admissions to three intensive care units (ICU) in a UK region from 2002 to 2006. Using a 21 day cut-off to define PMV, incidence was calculated using all ICU admissions and ventilated ICU admissions as denominators. Outcomes for the PMV cohort (mortality and hospital resource use) were compared with the non-PMV cohort. Length of ICU stay beyond 21 days was used to model the effect of establishing a weaning unit in terms of unit occupancy rates, admission refusal rates, and healthcare costs.
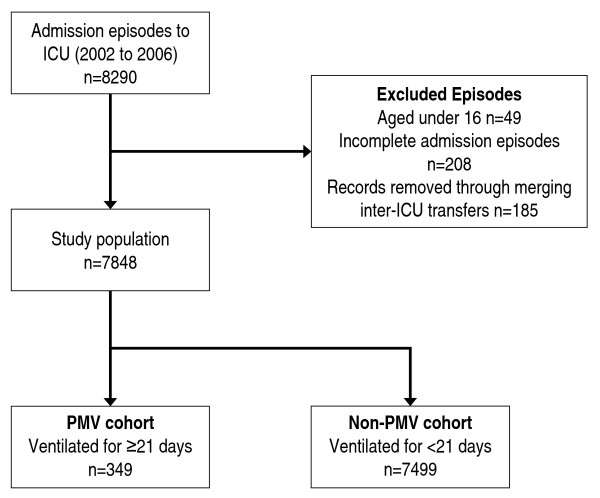
Results: Out of 8290 ICU admission episodes, 7848 were included in the analysis. Mechanical ventilation was required during 5552 admission episodes, of which 349 required PMV. The incidence of PMV was 4.4 per 100 ICU admissions, and 6.3 per 100 ventilated ICU admissions. PMV patients used 29.1% of all general ICU bed days, spent longer in hospital after ICU discharge than non-PMV patients (median 17 vs 7 days, P < 0.001) and had higher hospital mortality (40.3% vs 33.8%, P = 0.02). For the region, in which about 70 PMV patients were treated each year, a weaning unit with a capacity of three beds appeared most cost efficient, resulting in an occupancy rate of 73%, admission refusal rate at 21 days of 36%, and potential cost saving of £344,000 (€418,000) using UK healthcare tariffs.
Conclusions: One in every sixteen ventilated patients requires PMV in our region and this group use a substantial amount of health care resource. Establishing a weaning unit would potentially reduce acute bed occupancy by 8-10% and could reduce overall treatment costs. Restructuring the current configuration of critical care services to introduce weaning units should be considered if the expected increase in PMV incidence occurs.
Figures
References
-
- Comprehensive critical care: a review of adult critical care services. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
