

Low incidence of new biochemical and clinical hypogonadism following hypofractionated stereotactic body radiation therapy (SBRT) monotherapy for low- to intermediate-risk prostate cancer
- PMID: 21439088
- PMCID: PMC3083385
- DOI: 10.1186/1756-8722-4-12
Low incidence of new biochemical and clinical hypogonadism following hypofractionated stereotactic body radiation therapy (SBRT) monotherapy for low- to intermediate-risk prostate cancer
Abstract
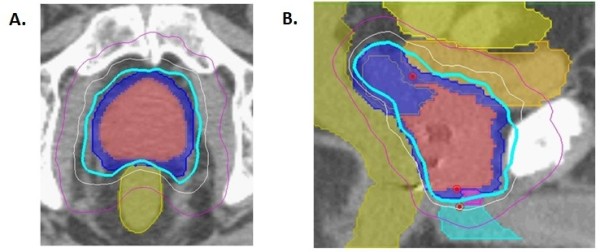
Background: The CyberKnife is an appealing delivery system for hypofractionated stereotactic body radiation therapy (SBRT) because of its ability to deliver highly conformal radiation therapy to moving targets. This conformity is achieved via 100s of non-coplanar radiation beams, which could potentially increase transitory testicular irradiation and result in post-therapy hypogonadism. We report on our early experience with CyberKnife SBRT for low- to intermediate-risk prostate cancer patients and assess the rate of inducing biochemical and clinical hypogonadism.
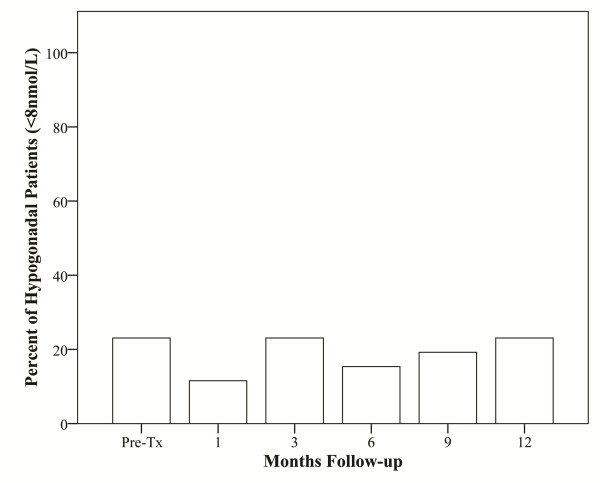
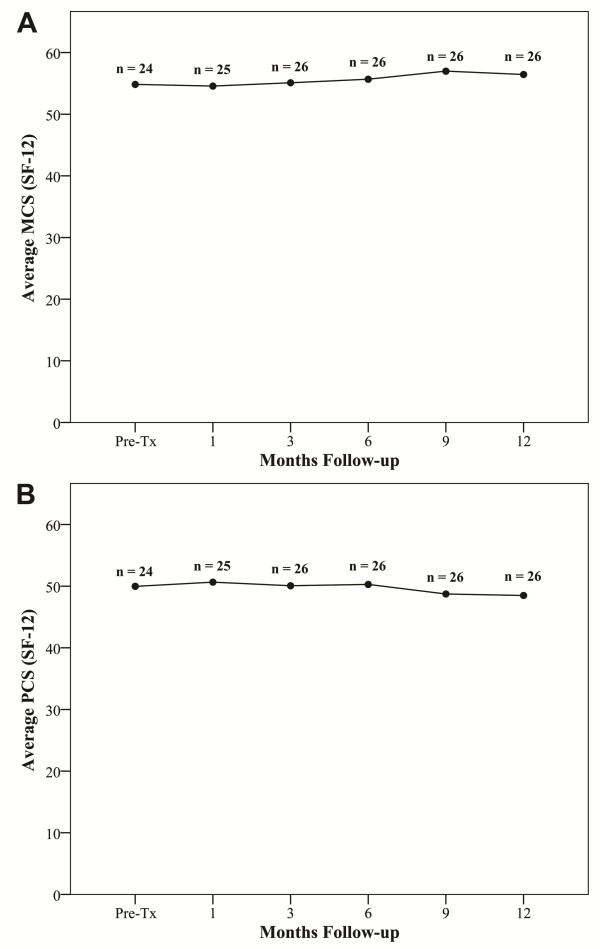
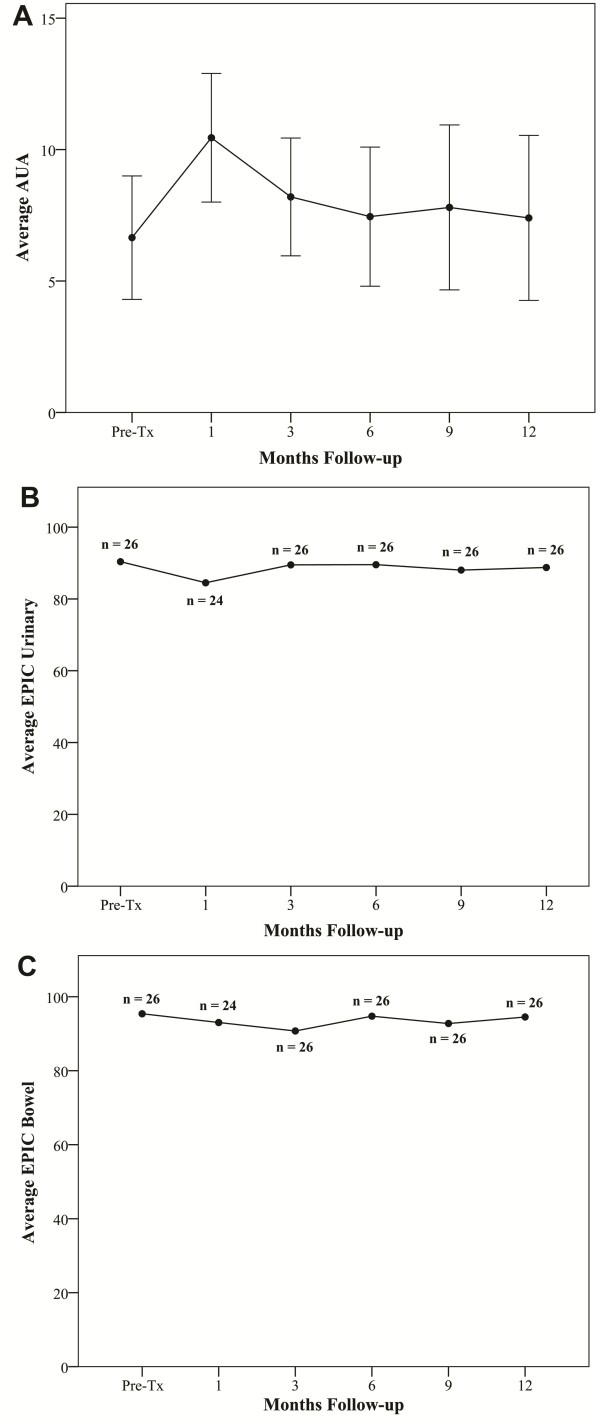
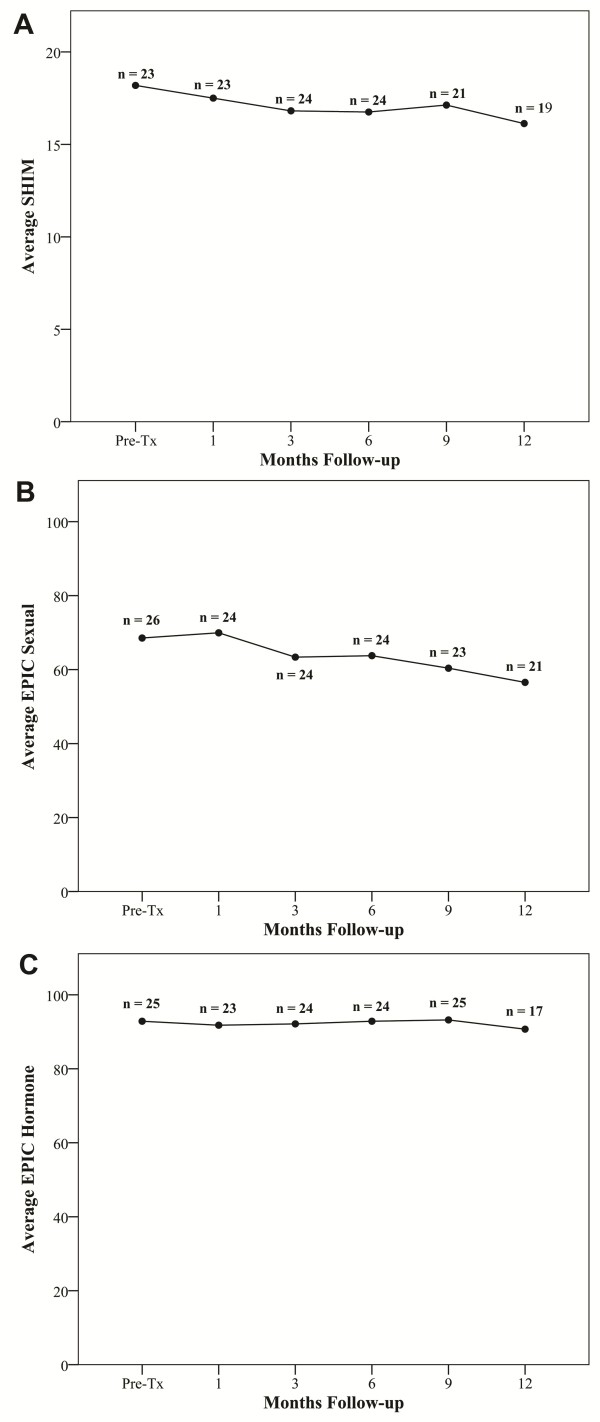
Methods: Twenty-six patients were treated with hypofractionated SBRT to a dose of 36.25 Gy in 5 fractions. All patients had histologically confirmed low- to intermediate-risk prostate adenocarcinoma (clinical stage ≤ T2b, Gleason score ≤ 7, PSA ≤ 20 ng/ml). PSA and total testosterone levels were obtained pre-treatment, 1 month post-treatment and every 3 months thereafter, for 1 year. Biochemical hypogonadism was defined as a total serum testosterone level below 8 nmol/L. Urinary and gastrointestinal toxicity was assessed using Common Toxicity Criteria v3; quality of life was assessed using the American Urological Association Symptom Score, Sexual Health Inventory for Men and Expanded Prostate Cancer Index Composite questionnaires.
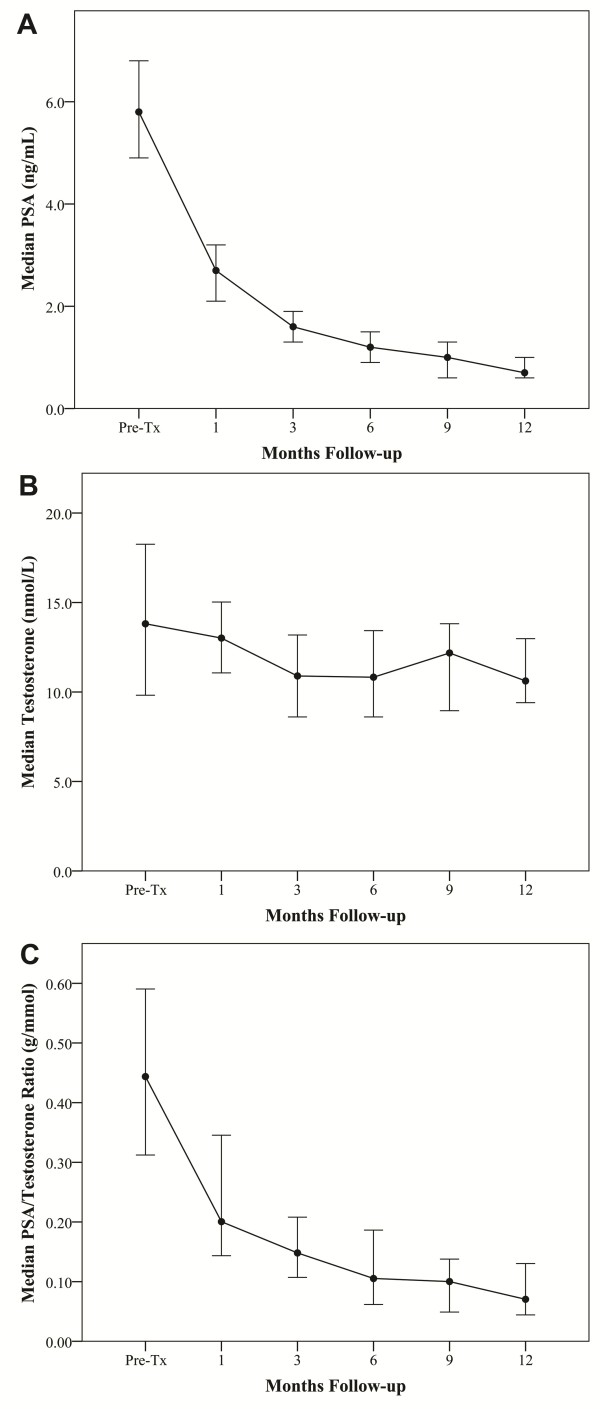
Results: All 26 patients completed the treatment with a median 15 months (range, 13-19 months) follow-up. Median pre-treatment PSA was 5.75 ng/ml (range, 2.3-10.3 ng/ml), and a decrease to a median of 0.7 ng/ml (range, 0.2-1.8 ng/ml) was observed by one year post-treatment. The median pre-treatment total serum testosterone level was 13.81 nmol/L (range, 5.55 - 39.87 nmol/L). Post-treatment testosterone levels slowly decreased with the median value at one year follow-up of 10.53 nmol/L, significantly lower than the pre-treatment value (p < 0.013). The median absolute fall was 3.28 nmol/L and the median percent fall was 23.75%. There was no increase in biochemical hypogonadism at one year post-treatment. Average EPIC sexual and hormonal scores were not significantly changed by one year post-treatment.
Conclusions: Hypofractionated SBRT offers the radiobiological benefit of a large fraction size and is well-tolerated by men with low- to intermediate-risk prostate cancer. Early results are encouraging with an excellent biochemical response. The rate of new biochemical and clinical hypogonadism was low one year after treatment.
Figures
References
-
- Kilby W, Dooley J, Kuduvalli G, Sayeh S, Maurer CRJ. The CyberKnife Robotic Radiosurgery System in 2010. Technol Cancer Res Treat. 2010;9:433–452. - PubMed
-
- Hossain S, Xia P, Huang K, Descovich M, Chuang C, Gottschalk AR, Roach M, Ma L. Dose Gradient Near Target-Normal Structure Interface for Nonisocentric CyberKnife and Isocentric Intensity-Modulated Body Radiotherapy for Prostate Cancer. Int J Radiat Oncol Biol Phys. in press . - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
