

Variation in management of immune suppression after allogeneic hematopoietic cell transplantation
- PMID: 21440079
- PMCID: PMC4497817
- DOI: 10.1016/j.bbmt.2011.03.006
Variation in management of immune suppression after allogeneic hematopoietic cell transplantation
Abstract
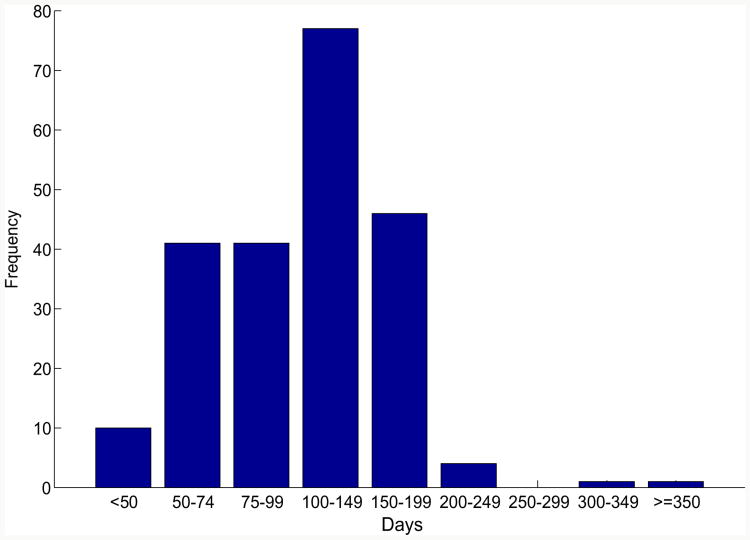
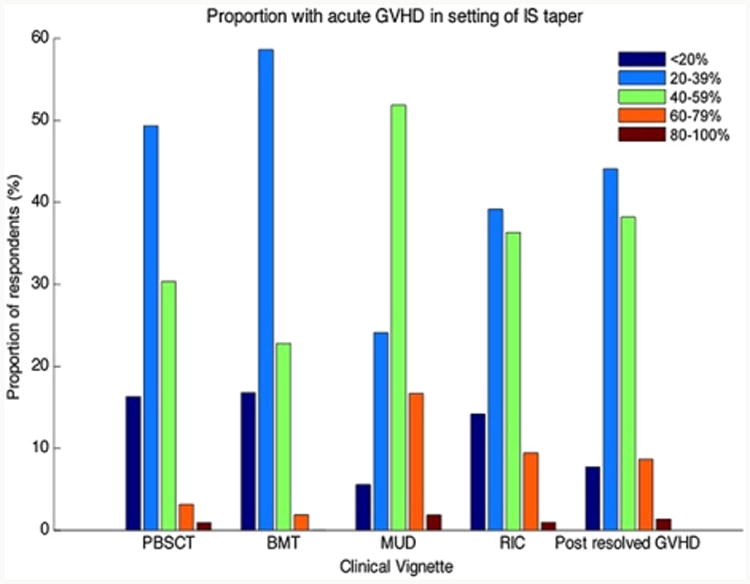
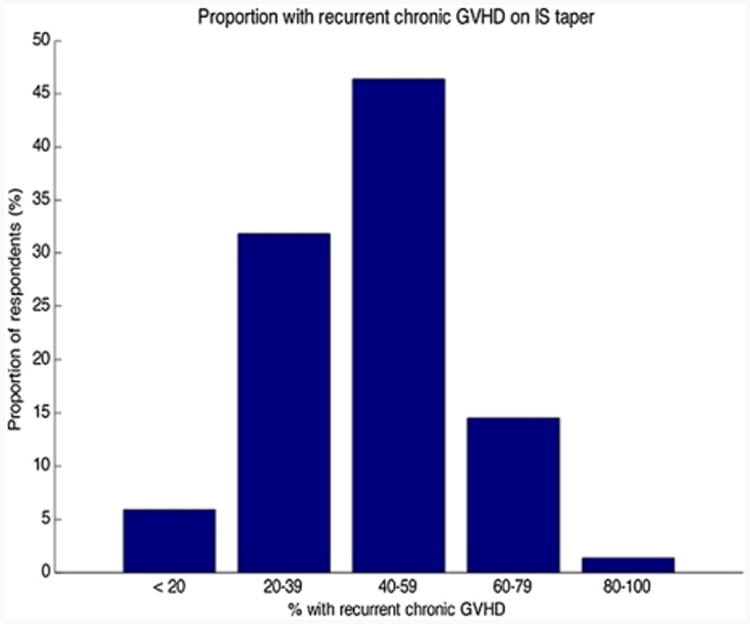
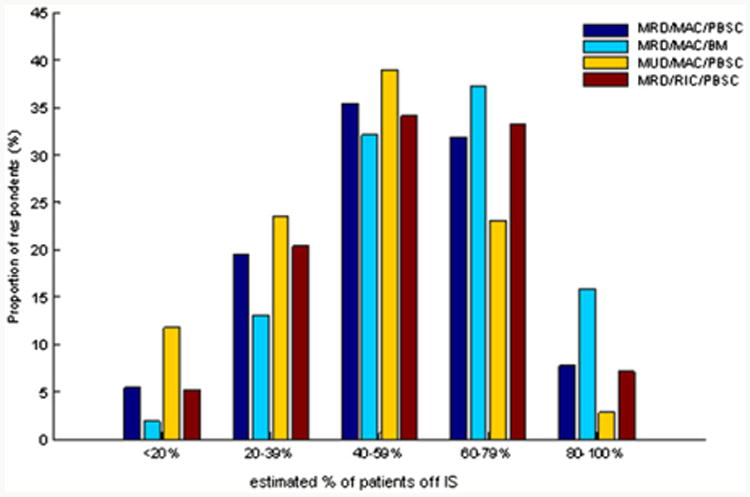
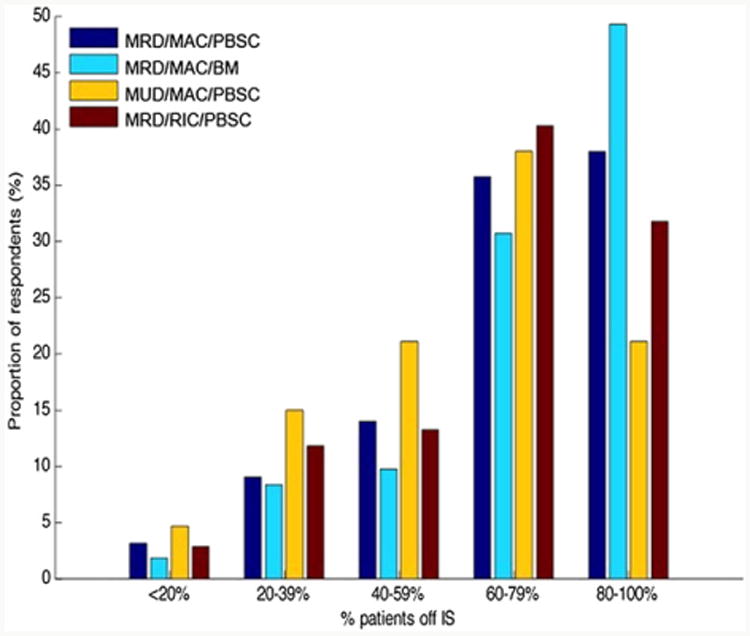
Practice variation in transplant physician management of immune suppression (IS) after allogeneic hematopoietic cell transplantation (HCT) is anticipated to have important consequences, but has not been characterized to date. We conducted a national survey of transplant physician members of the American Society for Blood and Marrow Transplantation to discern variation in IS management, characterize the burden of graft-versus-host disease (GVHD) emerging in the setting of IS taper, and describe the proportion of HCT recipients who successfully discontinue IS by 2 and 5 years post-HCT. There was marked heterogeneity in IS discontinuation practice, with variation in initiation of taper, sequence of agents tapered, frequency of changes, and strategy utilized. Twenty-five percent reported no consistent strategy in their usual practice. Confidence in therapeutic decision making was limited. The majority indicated that they could not predict who would develop GVHD on taper of IS, and reported a resultant burden of both acute and chronic GVHD (aGVHD, cGVHD) emerging or recurring in the setting of IS taper. HCT physicians projected rates of IS discontinuation that increased from 2 to 5 years post-HCT, and differed significantly according to donor relation and stem cell source utilized. The marked variation in practice, burden of GVHD emerging in the setting of IS taper, and limited confidence in therapeutic decision making all highlight shortcomings in an essential component of HCT physicians' scope of practice. These data argue for more rigorous study of IS management post-HCT so that evidence-based practice guidelines can be developed.
Copyright © 2011 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ratanatharathorn V, Nash RA, Przepiorka D, et al. Phase III study comparing methotrexate and tacrolimus (prograf, FK506) with methotrexate and cyclosporine for graft-versus-host disease prophylaxis after HLA-identical sibling bone marrow transplantation. Blood. 1998;92:2303–2314. - PubMed
-
- Nash RA, Antin JH, Karanes C, et al. Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood. 2000;96:2062–2068. - PubMed
-
- MacMillan ML, Weisdorf DJ, Wagner JE, et al. Response of 443 patients to steroids as primary therapy for acute graft-versus-host disease: comparison of grading systems. Biol Blood Marrow Transplant. 2002;8:387–394. - PubMed
-
- Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2003;9:215–233. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
