

Comparison of diagnostic accuracy of clinical measures of breast cancer-related lymphedema: area under the curve
- PMID: 21440706
- PMCID: PMC3698223
- DOI: 10.1016/j.apmr.2010.11.017
Comparison of diagnostic accuracy of clinical measures of breast cancer-related lymphedema: area under the curve
Abstract
Objective: To compare diagnostic accuracy of measures of breast cancer-related lymphedema (BCRL).
Design: Cross-sectional design comparing clinical measures with the criterion standard of previous diagnosis of BCRL.
Setting: University of California San Francisco Translational Science Clinical Research Center.
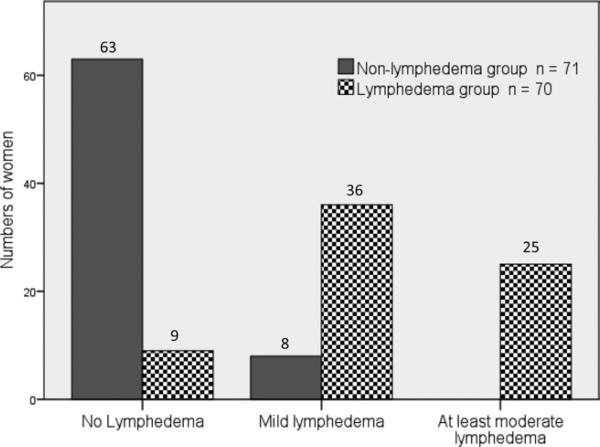
Participants: Women older than 18 years and more than 6 months posttreatment for breast cancer (n=141; 70 with BCRL, 71 without BCRL).
Interventions: Not applicable.
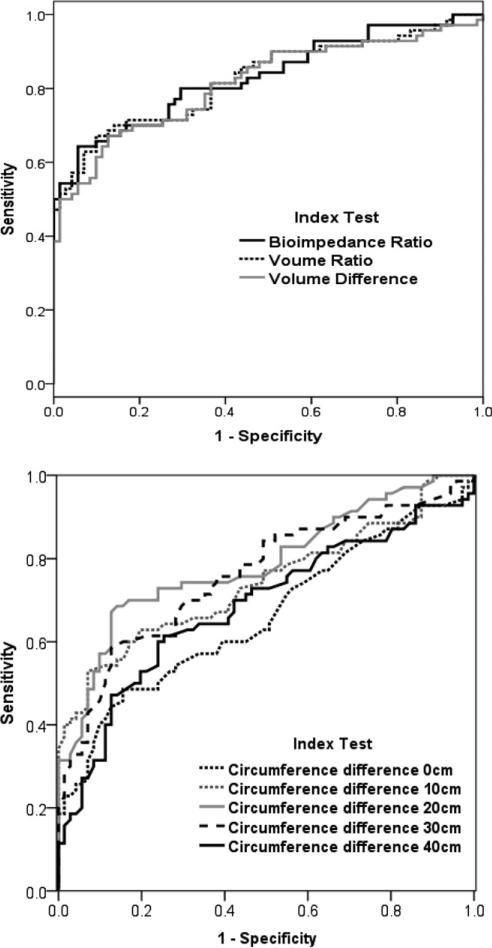
Main outcome measures: Sensitivity, specificity, receiver operator characteristic curve, and area under the curve (AUC) were used to evaluate accuracy.
Results: A total of 141 women were categorized as having (n=70) or not having (n=71) BCRL based on past diagnosis by a health care provider, which was used as the reference standard. Analyses of ROC curves for the continuous outcomes yielded AUC of .68 to .88 (P<.001); of the physical measures bioimpedance spectroscopy yielded the highest accuracy with an AUC of .88 (95% confidence interval, .80-.96) for women whose dominant arm was the affected arm. The lowest accuracy was found using the 2-cm diagnostic cutoff score to identify previously diagnosed BCRL (AUC, .54-.65).
Conclusions: Our findings support the use of bioimpedance spectroscopy in the assessment of existing BCRL. Refining diagnostic cutoff values may improve accuracy of diagnosis and warrant further investigation.
Copyright © 2011 American Congress of Rehabilitation Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Deo SV, Ray S, Rath GK, et al. Prevalence and risk factors for development of lymphedema following breast cancer treatment. Indian J Cancer. 2004;41:8–12. - PubMed
-
- Nardone L, Palazzoni G, D'Angelo E, et al. Impact of dose and volume on lymphedema. Rays. 2005;30:149–55. - PubMed
-
- Johansson K, Holmstrom H, Nilsson I, Ingvar C, Albertsson M, Ekdahl C. Breast cancer patients’ experiences of lymphoedema. Scand J Caring Sci. 2003;17:35–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
