

Cerebral perfusion pressure thresholds for brain tissue hypoxia and metabolic crisis after poor-grade subarachnoid hemorrhage
- PMID: 21441155
- PMCID: PMC3089891
- DOI: 10.1161/STROKEAHA.110.596874
Cerebral perfusion pressure thresholds for brain tissue hypoxia and metabolic crisis after poor-grade subarachnoid hemorrhage
Abstract
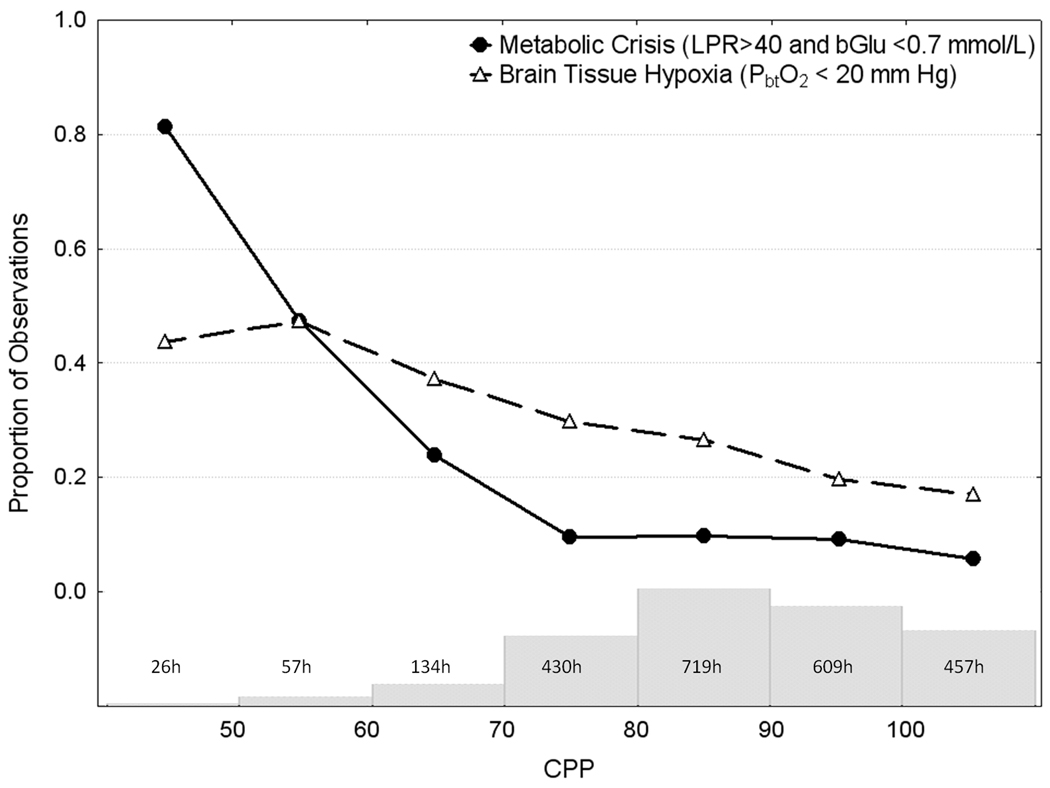
Background and purpose: To identify a minimally acceptable cerebral perfusion pressure threshold above which the risks of brain tissue hypoxia (BTH) and oxidative metabolic crisis are reduced for patients with subarachnoid hemorrhage (SAH).
Methods: We studied 30 poor-grade SAH patients who underwent brain multimodality monitoring (3042 hours). Physiological measures were averaged over 60 minutes for each collected microdialysis sample. Metabolic crisis was defined as a lactate/pyruvate ratio>40 with a brain glucose concentration≤0.7 mmol/L. BTH was defined as PbtO2<20 mm Hg. Outcome was assessed at 3 months with the Modified Rankin Scale.
Results: Multivariable analyses adjusting for admission Hunt-Hess grade, intraventricular hemorrhage, systemic glucose, and end-tidal CO2 revealed that cerebral perfusion pressure≤70 mm Hg was significantly associated with an increased risk of BTH (OR, 2.0; 95% CI, 1.2-3.3; P=0.007) and metabolic crisis (OR, 2.1; 95% CI, 1.2-3.7; P=0.007). Death or severe disability at 3 months was significantly associated with metabolic crisis (OR, 5.4; 95% CI, 1.8-16; P=0.002) and BTH (OR, 5.1; 95% CI, 1.2-23; P=0.03) after adjusting for admission Hunt-Hess grade.
Conclusions: Metabolic crisis and BTH are associated with mortality and poor functional recovery after SAH. Cerebral perfusion pressure levels<70 mm Hg was associated with metabolic crisis and BTH, and may increase the risk of secondary brain injury in poor-grade SAH patients.
Figures
References
-
- Raabe A, Beck J, Keller M, Vatter H, Zimmermann M, Seifert V. Relative importance of hypertension compared with hypervolemia for increasing cerebral oxygenation in patients with cerebral vasospasm after subarachnoid hemorrhage. Journal of Neurosurgery: Pediatrics. 2005:103. - PubMed
-
- Skjoth-Rasmussen J, Schulz M, Kristensen SR, Bjerre P. Delayed neurological deficits detected by an ischemic pattern in the extracellular cerebral metabolites in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2004;100:8–15. - PubMed
-
- Unterberg AW, Sakowitz OW, Sarrafzadeh AS, Benndorf G, Lanksch WR. Role of bedside microdialysis in the diagnosis of cerebral vasospasm following aneurysmal subarachnoid hemorrhage. J Neurosurg. 2001;94:740–749. - PubMed
-
- Ramakrishna R, Stiefel M, Udoetuk J, Spiotta A, Levine JM, Kofke WA, Zager E, Yang W, Leroux P. Brain oxygen tension and outcome in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2008;109:1075–1082. - PubMed
-
- Sarrafzadeh A, Haux D, Kuchler I, Lanksch WR, Unterberg AW. Poor-grade aneurysmal subarachnoid hemorrhage: Relationship of cerebral metabolism to outcome. J Neurosurg. 2004;100:400–406. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
