

Hypertension despite dehydration during severe pediatric diabetic ketoacidosis
- PMID: 21443581
- PMCID: PMC3103609
- DOI: 10.1111/j.1399-5448.2010.00695.x
Hypertension despite dehydration during severe pediatric diabetic ketoacidosis
Abstract
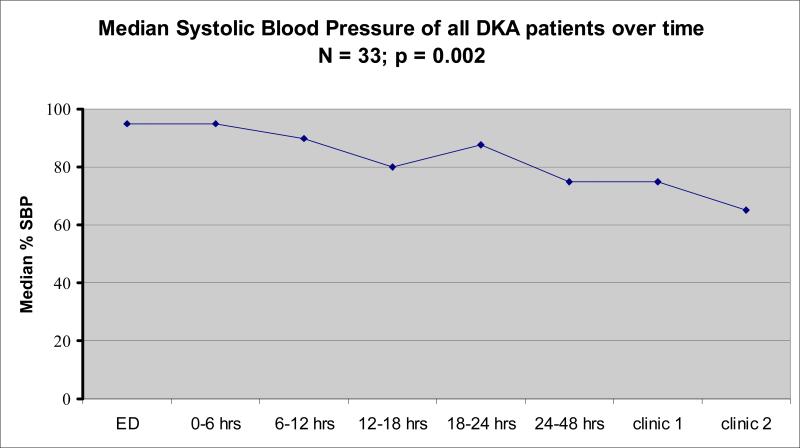
Objective: Diabetic ketoacidosis (DKA) may result in both dehydration and cerebral edema but these processes may have opposing effects on blood pressure. We examined the relationship between dehydration and blood pressure in pediatric DKA.
Design: A retrospective review was performed at Seattle Children's Hospital, Seattle, WA. Participants were hospitalized children less than 18 yr. Intervention(s) or main exposure was to patients with DKA (venous pH < 7.3, glucose > 300 mg/dL, HCO(3) < 15 mEq/L, and urinary ketosis). Dehydration was calculated as percent body weight lost at admission compared to discharge. Hypertension (systolic and/or diastolic blood pressure (DBP) percentile > 95%) was defined based on National Heart, Lung, and Blood Institute (NHLBI, 2004) nomograms and hypotension was defined as systolic blood pressure (SBP) <70 + 2 [age].
Results: Thirty-three patients (median 10.9 yr; range 10 months to 17 yr) were included. Fifty-eight percent of patients (19/33) had hypertension on admission before treatment and 82% had hypertension during the first 6 h of admission. None had admission hypotension. Hypertension 48 h after treatment and weeks after discharge was common (28 and 19%, respectively). Based on weight gained by discharge, 27% of patients had mild, 61% had moderate, and 12% presented with severe dehydration.
Conclusion: Despite dehydration, most children admitted with severe DKA had hypertension.
© 2011 John Wiley & Sons A/S.
Figures
Comment in
-
Diabetic ketoacidosis: persistence and paradox.Pediatr Diabetes. 2011 Jun;12(4 Pt 1):293-4. doi: 10.1111/j.1399-5448.2011.00787.x. Pediatr Diabetes. 2011. PMID: 21615649 No abstract available.
References
-
- Roche EF, Menon A, Gill D, Hoey H. Clinical presentation of type 1 diabetes. Pediatr Diabetes. 2005;6:75–78. - PubMed
-
- Wolfsdorf J, Craig ME, Daneman D, Dunger D, Edge J, Lee WRW, et al. Diabetic Ketoacidosis. Pediatr Diabetes. 2007;8:28–42. - PubMed
-
- Wolfsdorf J, Glaser N, Sperling MA. Diabetic ketoacidosis in infants, children, and adolescents: A consensus statement from the American Diabetes Association. Diabetes Care. 2006;29:1150–1159. - PubMed
-
- Glaser N, Barnett P, McCaslin I, et al. Risk factors for cerebral edema in children with diabetic ketoacidosis. The Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. N Engl J Med. 2001;344:264–269. - PubMed
-
- Brown FK. Cardiovascular effects of acutely raised intracranial pressure. Am J Physiol. 1956;185:510–14. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
