

Diagnosis, management, and outcomes of patients with syncope and bundle branch block
- PMID: 21444367
- PMCID: PMC3114095
- DOI: 10.1093/eurheartj/ehr071
Diagnosis, management, and outcomes of patients with syncope and bundle branch block
Abstract
Aims: Although patients with syncope and bundle branch block (BBB) are at high risk of developing atrio-ventricular block, syncope may be due to other aetiologies. We performed a prospective, observational study of the clinical outcomes of patients with syncope and BBB following a systematic diagnostic approach.
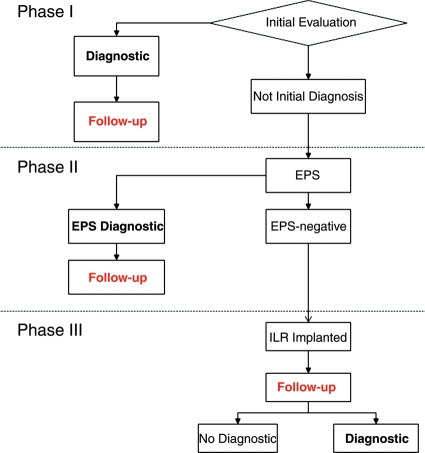
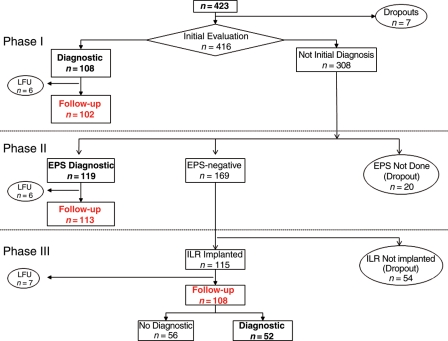
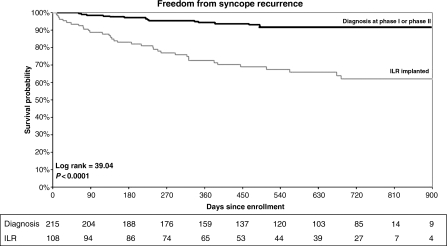
Methods and results: Patients with ≥1 syncope in the last 6 months, with QRS duration ≥120 ms, were prospectively studied following a three-phase diagnostic strategy: Phase I, initial evaluation; Phase II, electrophysiological study (EPS); and Phase III, insertion of an implantable loop recorder (ILR). Overall, 323 patients (left ventricular ejection fraction 56 ± 12%) were studied. The aetiological diagnosis was established in 267 (82.7%) patients (102 at initial evaluation, 113 upon EPS, and 52 upon ILR) with the following aetiologies: bradyarrhythmia (202), carotid sinus syndrome (20), ventricular tachycardia (18), neurally mediated (9), orthostatic hypotension (4), drug-induced (3), secondary to cardiopulmonary disease (2), supraventricular tachycardia (1), bradycardia-tachycardia (1), and non-arrhythmic (7). A pacemaker was implanted in 220 (68.1%), an implantable cardioverter defibrillator in 19 (5.8%), and radiofrequency catheter ablation was performed in 3 patients. Twenty patients (6%) had died at an average follow-up of 19.2 ± 8.2 months.
Conclusion: In patients with syncope, BBB, and mean left ventricular ejection fraction of 56 ± 12%, a systematic diagnostic approach achieves a high rate of aetiological diagnosis and allows to select specific treatment.
Figures
References
-
- McAnulty JH, Rahimtoola SH, Murphy E, DeMots H, Ritzmann L, Kanarek PE, Kauffman S. Natural history of high risk bundle branch block: final report of a prospective study. N Engl J Med. 1982;307:137–143. doi:10.1056/NEJM198207153070301. - DOI - PubMed
-
- Brignole M, Menozzi C, Moya A, Garcia-Civera R, Mont L, Alvarez M, Errazquin F, Beiras J, Bottoni N, Donateo P. Mechanism of syncope in patients with bundle branch block and negative electrophysiological test. Circulation. 2001;104:2045–2050. doi:10.1161/hc4201.097837. - DOI - PubMed
-
- Martin TP, Hanusa BH, Kapoor WN. Risk stratification of patients with syncope. Ann Emerg Med. 1997;29:459–466. doi:10.1016/S0196-0644(97)70217-8. - DOI - PubMed
-
- Colivicchi F, Ammirati F, Melina D, Guido V, Imperoli G, Santini M OESIL (Osservatorio Epidemiologico sulla Sincope nel Lazio) Study Investigators. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: the OESIL risk score. Eur Heart J. 2003;24:811–819. doi:10.1016/S0195-668X(02)00827-8. - DOI - PubMed
-
- Del Rosso A, Ungar A, Maggi R, Giada F, Petix NR, De Santo T, Menozzi C, Brignole M. Clinical predictors of cardiac syncope at initial evaluation in patients referred urgently to a general hospital: the EGSYS score. Heart. 2008;94:1620–1626. doi:10.1136/hrt.2008.143123. - DOI - PubMed
