

Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study
- PMID: 21444879
- PMCID: PMC3181498
- DOI: 10.1161/CIRCULATIONAHA.110.009035
Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study
Abstract
Background: Atrial fibrillation (AF) is an important risk factor for stroke and overall mortality, but information about the preventable burden of AF is lacking. The aim of this study was to determine what proportion of the burden of AF in blacks and whites could theoretically be avoided by the maintenance of an optimal risk profile.
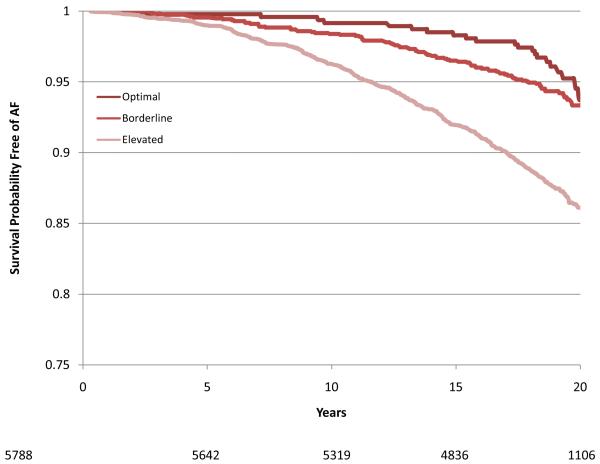
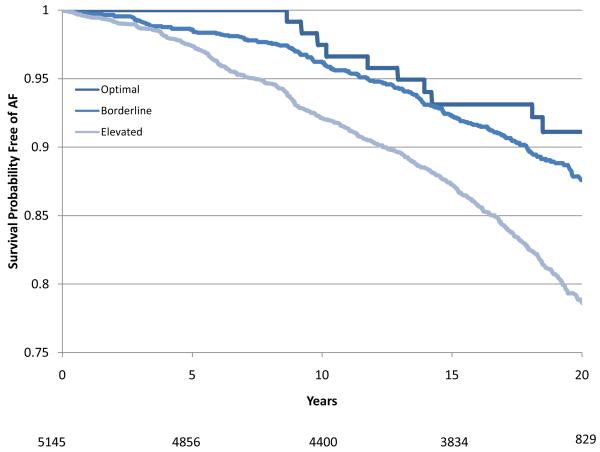
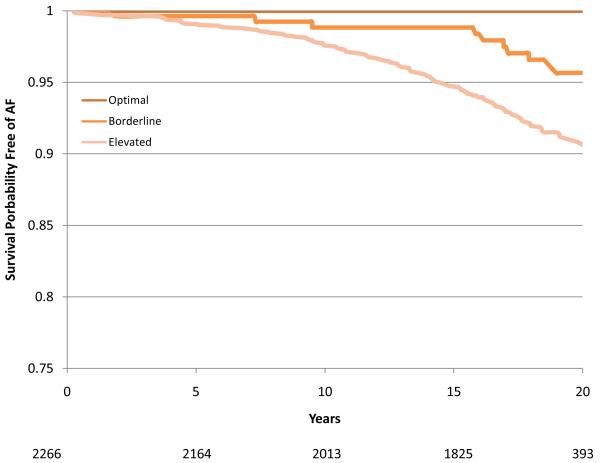
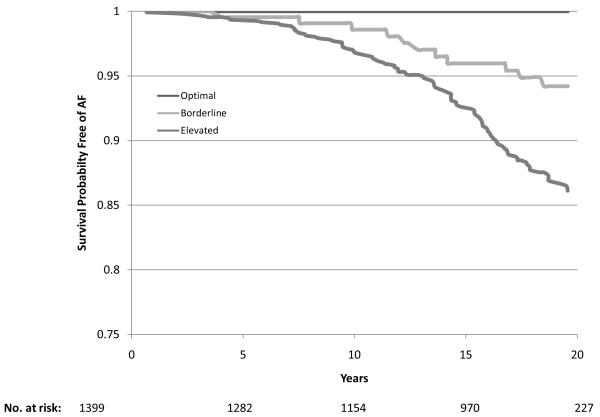
Methods and results: This study included 14 598 middle-aged Atherosclerosis Risk in Communities (ARIC) Study cohort members. Previously established AF risk factors, namely high blood pressure, elevated body mass index, diabetes mellitus, cigarette smoking, and prior cardiac disease, were categorized into optimal, borderline, and elevated levels. On the basis of their risk factor levels, individuals were classified into 1 of these 3 groups. The population-attributable fraction of AF resulting from having a nonoptimal risk profile was estimated separately for black and white men and women. During a mean follow-up of 17.1 years, 1520 cases of incident AF were identified. The age-adjusted incidence rates were highest in white men and lowest in black women (7.45 and 3.67 per 1000 person-years, respectively). The overall prevalence of an optimal risk profile was 5.4% but varied according to race and gender: 10% in white women versus 1.6% in black men. Overall, 56.5% of AF cases could be explained by having ≥ 1 borderline or elevated risk factors, of which elevated blood pressure was the most important contributor.
Conclusion: As with other forms of cardiovascular disease, more than half of the AF burden is potentially avoidable through the optimization of cardiovascular risk factors levels.
Figures
References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–5. - PubMed
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O’Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y, American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146. - PubMed
-
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–52. - PubMed
-
- Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds MR, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health. 2006;9:348–356. - PubMed
-
- Benjamin EJ, Chen PS, Bild DE, Mascette AM, Albert CM, Alonso A, Calkins H, Connolly SJ, Curtis AB, Darbar D, Ellinor PT, Go AS, Goldschlager NF, Heckbert SR, Jalife J, Kerr CR, Levy D, Lloyd-Jones DM, Massie BM, Nattel S, Olgin JE, Packer DL, Po SS, Tsang TS, Van Wagoner DR, Waldo AL, Wyse DG. Prevention of atrial fibrillation: report from a National Heart, Lung, and Blood Institute Workshop. Circulation. 2009;119:606–18. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC055022/HC/NHLBI NIH HHS/United States
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01 HC055019/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- RC1 HL099452/HL/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- N01 HC055015/HC/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- N01 HC055016/HC/NHLBI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- RC1-HL09945/HL/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01 HC055019/HC/NHLBI NIH HHS/United States
- N01 HC055021/HC/NHLBI NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01 HC055020/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
