

A new Web-based medical tool for assessment and prevention of comprehensive cardiovascular risk
- PMID: 21445280
- PMCID: PMC3061845
- DOI: 10.2147/TCRM.S16523
A new Web-based medical tool for assessment and prevention of comprehensive cardiovascular risk
Abstract
Background: Multifactor cardiovascular disease is the leading cause of death; besides well-known cardiovascular risk factors, several emerging factors such as mental stress, diet type, and physical inactivity, have been associated to cardiovascular disease. To date, preventive strategies are based on the concept of absolute risk calculated by different algorithms and scoring systems. However, in general practice the patient's data collection represents a critical issue.
Design: A new multipurpose computer-based program has been developed in order to:1) easily calculate and compare the absolute cardiovascular risk by the Framingham, Procam, and Progetto Cuore algorithms; 2) to design a web-based computerized tool for prospective collection of structured data; 3) to support the doctor in the decision-making process for patients at risk according to recent international guidelines.
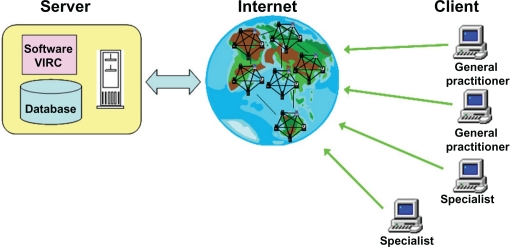
Methods: During a medical consultation the doctor utilizes a common computer connected by Internet to a medical server where all the patient's data and software reside. The program evaluates absolute and relative cardiovascular risk factors, personalized patient's goals, and multiparametric trends, monitors critical parameter values, and generates an automated medical report.
Results: In a pilot study on 294 patients (47% males; mean age 60 ± 12 years [±SD]) the global time to collect data at first consultation was 13 ± 11 minutes which declined to 8 ± 7 minutes at the subsequent consultation. In 48.2% of cases the program revealed 2 or more primary risk factor parameters outside guideline indications and gave specific clinical suggestions to return altered parameters to target values.
Conclusion: The web-based system proposed here may represent a feasible and flexible tool for clinical management of patients at risk of cardiovascular disease and for epidemiological research.
Keywords: cardiovascular risk; clinical information systems; decision support; evidence-based practice; informatics; internet; medical consultation.
Figures








References
-
- De Backer G, Ambrosioni E, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice. Eur J Cardiovasc Prev Rehabil. 2003;10:S1–S78. - PubMed
-
- Sidney C, Smith, Allen J, et al. AHA/ACC Guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update. J Am Coll Cardiol. 2006;47:2130–2139. - PubMed
-
- Holmes JS, Arispe IE, Moy E. Heart disease and prevention: race and age differences in heart disease, prevention, treatment and mortality. Med Care. 2005;43:I33–I41. - PubMed
-
- Smith SC, Jr, Blair SN, Bonow RO, et al. AHA/ACC guidelines for preventing heart attack and death in patients with atherosclerotic cardiovascular disease: 2001 update: A statement for healthcare professionals from the American Heart Association and the American College of Cardiology. Circulation. 2001;104:1577–1579. - PubMed
-
- Hopkins PN, Williams RR. Identification and relative weight of cardiovascular risk factors. Cardiol Clin. 1986;4:3–31. - PubMed
LinkOut - more resources
Full Text Sources
