

Scaling up diarrhea prevention and treatment interventions: a Lives Saved Tool analysis
- PMID: 21445330
- PMCID: PMC3062532
- DOI: 10.1371/journal.pmed.1000428
Scaling up diarrhea prevention and treatment interventions: a Lives Saved Tool analysis
Abstract
Background: Diarrhea remains a leading cause of mortality among young children in low- and middle-income countries. Although the evidence for individual diarrhea prevention and treatment interventions is solid, the effect a comprehensive scale-up effort would have on diarrhea mortality has not been estimated.
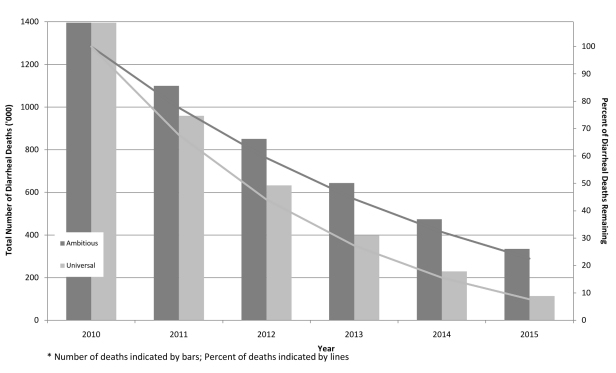
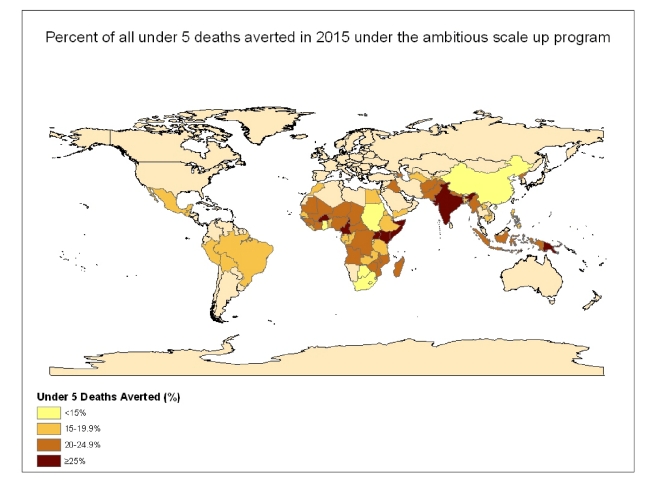
Methods and findings: We use the Lives Saved Tool (LiST) to estimate the potential lives saved if two scale-up scenarios for key diarrhea interventions (oral rehydration salts [ORS], zinc, antibiotics for dysentery, rotavirus vaccine, vitamin A supplementation, basic water, sanitation, hygiene, and breastfeeding) were implemented in the 68 high child mortality countries. We also conduct a simple costing exercise to estimate cost per capita and total costs for each scale-up scenario. Under the ambitious (feasible improvement in coverage of all interventions) and universal (assumes near 100% coverage of all interventions) scale-up scenarios, we demonstrate that diarrhea mortality can be reduced by 78% and 92%, respectively. With universal coverage nearly 5 million diarrheal deaths could be averted during the 5-year scale-up period for an additional cost of US$12.5 billion invested across 68 priority countries for individual-level prevention and treatment interventions, and an additional US$84.8 billion would be required for the addition of all water and sanitation interventions.
Conclusion: Using currently available interventions, we demonstrate that with improved coverage, diarrheal deaths can be drastically reduced. If delivery strategy bottlenecks can be overcome and the international community can collectively deliver on the key strategies outlined in these scenarios, we will be one step closer to achieving success for the United Nations' Millennium Development Goal 4 (MDG4) by 2015.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375:1969–1987. - PubMed
-
- UNICEFWHO. Geneva: WHO; 2009. Diarrhoea: why children are still dying and what can be done. - PubMed
-
- UNICEF. New York: UNICEF; 2008. Tracking progress in maternal, newborn and child survival.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
