

Multicenter evaluation of a novel surveillance paradigm for complications of mechanical ventilation
- PMID: 21445364
- PMCID: PMC3062570
- DOI: 10.1371/journal.pone.0018062
Multicenter evaluation of a novel surveillance paradigm for complications of mechanical ventilation
Abstract
Background: Ventilator-associated pneumonia (VAP) surveillance is time consuming, subjective, inaccurate, and inconsistently predicts outcomes. Shifting surveillance from pneumonia in particular to complications in general might circumvent the VAP definition's subjectivity and inaccuracy, facilitate electronic assessment, make interfacility comparisons more meaningful, and encourage broader prevention strategies. We therefore evaluated a novel surveillance paradigm for ventilator-associated complications (VAC) defined by sustained increases in patients' ventilator settings after a period of stable or decreasing support.
Methods: We assessed 600 mechanically ventilated medical and surgical patients from three hospitals. Each hospital contributed 100 randomly selected patients ventilated 2-7 days and 100 patients ventilated >7 days. All patients were independently assessed for VAP and for VAC. We compared incidence-density, duration of mechanical ventilation, intensive care and hospital lengths of stay, hospital mortality, and time required for surveillance for VAP and for VAC. A subset of patients with VAP and VAC were independently reviewed by a physician to determine possible etiology.
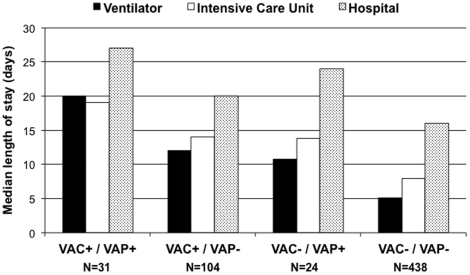
Results: Of 597 evaluable patients, 9.3% had VAP (8.8 per 1,000 ventilator days) and 23% had VAC (21.2 per 1,000 ventilator days). Compared to matched controls, both VAP and VAC prolonged days to extubation (5.8, 95% CI 4.2-8.0 and 6.0, 95% CI 5.1-7.1 respectively), days to intensive care discharge (5.7, 95% CI 4.2-7.7 and 5.0, 95% CI 4.1-5.9), and days to hospital discharge (4.7, 95% CI 2.6-7.5 and 3.0, 95% CI 2.1-4.0). VAC was associated with increased mortality (OR 2.0, 95% CI 1.3-3.2) but VAP was not (OR 1.1, 95% CI 0.5-2.4). VAC assessment was faster (mean 1.8 versus 39 minutes per patient). Both VAP and VAC events were predominantly attributable to pneumonia, pulmonary edema, ARDS, and atelectasis.
Conclusions: Screening ventilator settings for VAC captures a similar set of complications to traditional VAP surveillance but is faster, more objective, and a superior predictor of outcomes.
Conflict of interest statement
Figures
References
-
- Klompas M, Platt R. Ventilator-associated pneumonia–the wrong quality measure for benchmarking. Ann Intern Med. 2007;147:803–805. - PubMed
-
- Uckay I, Ahmed QA, Sax H, Pittet D. Ventilator-associated pneumonia as a quality indicator for patient safety? Clin Infect Dis. 2008;46:557–563. - PubMed
-
- Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–332. - PubMed
-
- Fagon JY, Chastre J, Hance AJ, Domart Y, Trouillet JL, et al. Evaluation of clinical judgment in the identification and treatment of nosocomial pneumonia in ventilated patients. Chest. 1993;103:547–553. - PubMed
-
- Schurink CA, Van Nieuwenhoven CA, Jacobs JA, Rozenberg-Arska M, Joore HC, et al. Clinical pulmonary infection score for ventilator-associated pneumonia: accuracy and inter-observer variability. Intensive Care Med. 2004;30:217–224. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
