

Effect of problem-solving-based diabetes self-management training on diabetes control in a low income patient sample
- PMID: 21445680
- PMCID: PMC3157525
- DOI: 10.1007/s11606-011-1689-6
Effect of problem-solving-based diabetes self-management training on diabetes control in a low income patient sample
Abstract
Background: Lower socioeconomic status is associated with excess disease burden from diabetes. Diabetes self-management support interventions are needed that are effective in engaging lower income patients, addressing competing life priorities and barriers to self-care, and facilitating behavior change.
Objective: To pilot test feasibility, acceptability, and effect on disease control of a problem-based diabetes self-management training adapted for low literacy and accessibility.
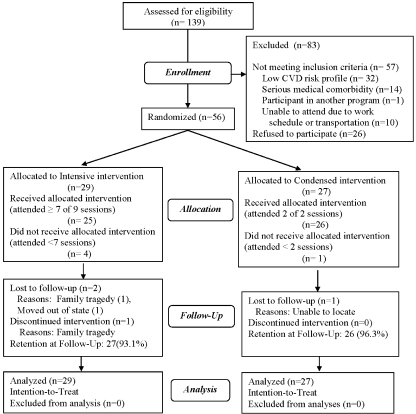
Design: Two-arm randomized controlled trial powered to detect a 0.50% change in A1C at follow-up with a 2-sided alpha of 0.05 in a pooled analysis.
Participants: Fifty-six urban African-American patients with type 2 diabetes and suboptimal blood sugar, blood pressure, or cholesterol control recruited from a diabetes registry within a university-affiliated managed care organization.
Interventions: A group, problem-based diabetes self-management training designed for delivery in an intensive and a condensed program format. Three intensive and three condensed program groups were conducted during the trial.
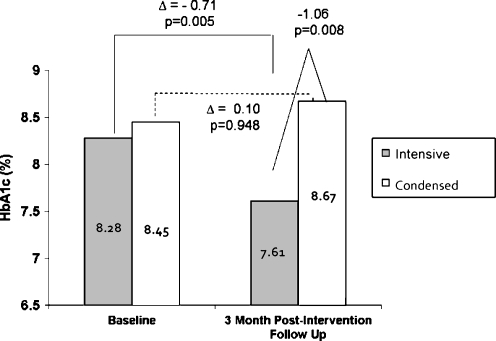
Main measures: Clinical (A1C, systolic blood pressure [SBP], diastolic blood pressure [DBP], LDL and HDL cholesterol) and behavioral (knowledge, problem solving, self-management behavior) data were measured at baseline, post-intervention, and 3 months post-intervention (corresponding with 6-9 months following baseline).
Results: Adoption of both programs was high (>85% attendance rates, 95% retention). At 3 months post-intervention, the between-group difference in A1C change was -0.72% (p = 0.02), in favor of the intensive program. A1C reduction was partially mediated by problem-solving skill at follow-up (ß = -0.13, p = 0.04). Intensive program patients demonstrated within-group improvements in knowledge (p < 0.001), problem-solving (p = 0.01), and self-management behaviors (p = 0.04). Among the subsets of patients with suboptimal blood pressure or lipids at baseline, the intensive program yielded clinically significant individual improvements in SBP, DBP, and LDL cholesterol. Patient satisfaction and usability ratings were high for both programs.
Conclusions: A literacy-adapted, intensive, problem-solving-based diabetes self-management training was effective for key clinical and behavioral outcomes in a lower income patient sample.
Trial registration: ClinicalTrials.gov NCT00201110.
Figures
Comment in
-
Optimizing diabetes self-care in low literacy and minority populations--problem-solving, empowerment, peer support and technology-based approaches.J Gen Intern Med. 2011 Sep;26(9):953-5. doi: 10.1007/s11606-011-1759-9. J Gen Intern Med. 2011. PMID: 21647745 Free PMC article. No abstract available.
References
-
- Priority areas for national action: Transforming health care quality. Washington, D.C.: National Academies Press; 2003. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
